
Emerging Infectious Diseases and Diagnosis Journal
Research Article
Knowledge, Attitude and Practices of University Students towards Prevention of Dengue in Northern India: A Questionnaire-Based Study
Prashar PK1, Dutta S1, Neha1, Kumar B1, Taylor-Robinson AW 2 and Amarjeet Singh3*
1School of Pharmaceutical Sciences, Lovely Professional University, Jalandhar, India
2School of Health, Medical & Applied Sciences, Central Queensland University, Brisbane, Australia
3Parexel International India Pvt. Ltd, India
*Corresponding author: Amarjeet Singh, Parexel International India Pvt. Ltd, India, Tel: +918289000296, Email: amarjeet31890@yahoo.in
Citation: Prashar PK, Dutta S, Neha, Kumar B, Taylor-Robinson AW and Amarjeet Singh (2019) Knowledge, Attitude and Practices of University Students towards Prevention of Dengue in Northern India: A Questionnaire-Based Study. Emerg Infect Dis Diag J: EIDDJ-100002
Received date: 22 June, 2019; Accepted date: 27 August, 2019; Published date: 03 September 2019
Abstract
Background: Dengue is one of the most common arthropod-borne (arbo) viral diseases of humans and poses an increasing global public health threat. Outbreaks of dengue infection in Punjab, India, have been reported for many years, with local transmission by Aedes mosquitoes resulting in multiple case reports in the north west of the state.
Objective: This study aimed to assess the knowledge, attitude and practice (KAP) of university students towards dengue in order to inform implementation of intervention strategies for an effective dengue prevention program.
Materials and Methods: A descriptive cross-sectional study was conducted on 450 undergraduate and postgraduate students using a pre-tested, self-administered, structured questionnaire. A targeted sampling method was used to enroll respondents at universities in the cities of Ludhiana and Jalandhar. Responses to a range of questions evaluated each participant’s knowledge, attitude and practice towards dengue. The collected data were tabulated and analyzed using Statistical Package for Social Sciences software.
Results: The findings indicate that 38.6% (174/450) of respondents had poor knowledge regarding dengue. Awareness was greater among those studying for a higher academic degree. More than half of participants (249/450; 55.3%) had not attended a workshop or received any other type of formal training relating to prevention of dengue. Approximately one-third of the study cohort did not appreciate the relevance to mosquito control of at least weekly draining ditches (171/450; 38.0%) or of regularly emptying water-filled containers (141/450; 31.3%).
Conclusion: The study suggests an apparent lack of knowledge of university students regarding dengue. The insufficiently serious attitude described by many reflects an inadequate level of awareness of dengue. The preventive measures taken by participants were often not effective practices. Hence, the study indicates that future dengue awareness campaigns are required to increase KAP levels and that these should target academic institutions, among other communities, in urban areas of Punjab. These findings may have wider relevance to any region in which dengue is endemic.
Keywords: Aedes; Attitude; Control; Dengue; India; knowledge; Practice; Prevention; Punjab
Introduction
Dengue is the most widespread vector-borne infectious disease of humans. Over half of the world’s population now live in tropical and subtropical zones that places them at risk of infection [1]. There are an estimated 400 million infections per annum, of which a quarter may manifest clinically, in close to 130 countries worldwide [2]. This leads to more than 500,000 hospitalizations, mainly among children [3]. The annual average number of dengue cases reported to the World Health Organization (WHO) has increased dramatically in recent years. For the period 2000-2004, the annual average was 925,896 cases globally, almost twice the figure of 479,848 cases that was reported during 1990-1999 [4]. In India, more than 10,000 cases were reported in 2014, which was doubled in 2015 [5]. Since the first outbreak in 1963 in Calcutta, since renamed Kolkata, dengue has occurred in most Indian regions. For 2016, 27 of 35 states and union territories reported the clinical incidence of dengue [6]. The causative agent of the disease is a single-stranded positive-sense RNA virus, DENV, a member of the genus Flavivirus and family Flaviviridae. Based on differences in antigen neutralization tests, there are four formally recognized, closely related serotypes of the dengue virus, DENV-1 to DENV-4 [7,8].
DENV is transmitted between humans primarily by infectious mosquitoes of the species Aedes aegypti and Ae. albopictus that are endemic to tropical countries [9]. Both show a preference for day-biting, with Ae. aegypti being considered a particular pest due to its peridomestic habitat. Clinical symptoms are a sudden-onset fever, headache (typically behind the eyes), myalgia, arthralgia, and a flat red rash [10]. The alternative name for dengue, ‘break-bone fever’, comes from the associated muscle and joints pains. The course of infection is divided into three phases; febrile, critical and recovery. The febrile phase usually lasts 2-7 days, is characterized by high fever, frequently over 40°C (104°F), and is associated with generalized pain and a headache. Flushed skin and small red spots called petechiae, which are caused by broken capillaries, may appear at this point. The critical phase, if it occurs, follows the resolution of high fever and typically lasts 1-2 days [10]. There may be significant fluid accumulation in the chest and abdominal cavity due to increased capillary permeability and leakage. This leads to depletion of fluid from the circulation and organs. Organ dysfunction and severe bleeding (typically from the gastrointestinal tract) may also occur. Shock and haemorrhage eventuate in less than 5% of all cases of dengue but those who experience a secondary infection with a DENV serotype different to that which caused primary infection are at an increased risk [11].
Laboratory methods to confirm a diagnosis of dengue infection may involve detection of the virus, viral nucleic acid, antigens or antibodies, or a combination of these techniques [12,13]. Despite decades of research, the continuing unavailability of an effective antiviral drug and/or licensed vaccine makes dengue a major global public health priority [14]. In the absence of therapeutic interventions, disease prevention is currently restricted to mosquito control [15]. Although several promising methods exist the way in which vector control programs are implemented has failed to prevent dengue epidemics and the expansion of Aedes over a wide geographical distribution [16]. Limitations of existing strategies include dwindling financial resources, development of insecticide resistance by mosquitoes, failure of long-term sustainability and lack of community engagement [17]. This has led the WHO to recommend a policy of integrated vector management that aims at using multiple mosquito control methods simultaneously to target several vector-borne diseases [9].
In order to determine an effective integrated control measure, it is critically important to evaluate the level of community awareness as well as to identify the measures that people commonly adopt [18]; this was the primary goal of the survey performed on university students, a supposedly well-educated sector of society [19]. The findings hold pragmatic value to policy makers of Punjab for implementing a public health information drive to assist in the reduction, and ultimately prevention, of dengue. This will help to establish where efforts need to be focused in future, not only in India, but also in neighbouring countries where arboviral infections pose an increasing threat to public health [20].
Materials and Methods
Study Design, Settings and Study Subjects: A cross-sectional study was conducted in Ludhiana and Jalandhar, two of the three largest cities of the northern Indian state of Punjab. The study commenced at the start of August 2017 and continued for four months (Table 1).
The research methodology, consent forms and set of questions all received prior approval from the project review committee of Lovely Professional University, Jalandhar, Punjab. All research staff involved in the study were required to sign a confidentiality statement before the commencement of data collection. Recruitment of survey respondents was undertaken on higher education campuses. Each was asked to complete a structured questionnaire provided in person by a member of a team of experienced trained operators. Verbal and written informed consent was obtained from all study subjects. Participants retained their anonymity but were requested to show proof of student status (valid photographic identification card, or similar).
The subjects were taught students of Diploma, Bachelors and Masters qualifications as well as PhD research scholars of various academic streams (engineering, business, arts, medical sciences, etc.) from several colleges and universities in Ludhiana and Jalandhar. Our research hypothesis was that awareness of dengue is influenced by the level and stream of academic study of an individual.
Sampling and Sample Size Calculation: A targeted sampling technique was used to recruit a sample size of 450 participants at different higher educational institutes in Ludhiana and Jalandhar.
Questionnaire
Following a thorough literature survey of dengue incidence, epidemiology and control in India and elsewhere a first draft questionnaire was prepared that consisted of two sets of standard questions. The first set gathered sociodemographic information about each participant, including their gender, age, educational status and academic stream. The second set contained a total of 30 questions that assessed three main themes: (1) the knowledge of the subject regarding dengue; (2) the attitude of the subject towards dengue; and (3) the practice of the subject regarding prevention methods for dengue. An information sheet was attached to each questionnaire that provided a short description of the aims of the study and instructions on how to complete and return the form.
The content of the questionnaire was validated by two professionally qualified academicians, faculty members of the School of Pharmaceutical Sciences, Lovely Professional University. After making revisions suggested by these discipline-specific experts, a pilot test was performed using a sample of 30 randomly selected students. Minor amendments to improve text of questions were made after review of pre-test frequency distributions and feedback (e.g. comments on effect of question order on responses, inappropriate response categories, ambiguous wording). Further to this evaluation, a final version of the questionnaire was prepared and approved for use in the full-scale study.
Statistical Analysis: A descriptive analysis of validated and compiled data was performed using statistical package for social science (SPSS, version 17) and MS Excel.
Results
Demographic Details of Respondents: The personal details of the subjects enrolled in the study were categorized according to age, gender, living status, educational level and educational study stream (Table 2). Of 450 approached participants who enrolled in the study, a majority of respondents (241; 53.6%) were between 21-25 years old. More than half of all participants (267/450; 59.3%) were males. Approximately two-thirds of respondents (294/450; 65.3%) were residents of urban areas. Around half the subjects (242/450; 53.8%) were undergraduate students, approximately one-quarter of subjects (105/450; 23.3%) were studying postgraduate courses, around one-fifth of participants were diploma students (80/450; 17.8%), while PhD scholars comprised a smaller enrolment group (23/450; 5.1%). Almost one-third of respondents (140/450; 31.1%) were studying engineering, about one-quarter (114/450; 25.3%) business and management, and nearly one-fifth (83/450; 18.4%) applied medical science. Arts and design students and participants enrolled in other related streams of study made up 8.7% (39/450) and 16.7% (74/450) of the cohort, respectively. There was no significant difference in the views of respondents based on variables in each of the demographic categories (P > 0.05).
Assessment of Knowledge of Respondents regarding Dengue: In order to assess knowledge regarding dengue, participants were asked to answer a set of ten questions about the mode of spread of dengue, the mosquito species responsible for dengue transmission, prevalence of dengue with respect to different seasons, and similar topics (Table 3).
More than two-thirds of subjects (302/450; 67.1%) were not able to determine the correct mode of spread of dengue. In responding to a related question, almost three-fifths (267/450; 59.3%) of participants were not aware that mosquitoes are responsible for transmission of dengue. A similar proportion (263/450; 58.4%) were not aware of the variation in prevalence of dengue during different climatic seasons.
The responses of all participants to the questions shown in Table 3 were used to generate a knowledge score for each student. Scores were ranked on an arbitrary scale from 1 to 10, with one mark allocated for each answer. In order to reflect knowledge of dengue scores were divided into three categories: 1) poor (0-4 marks); 2) moderate (5-6 marks); and good (7-10 marks). This demonstrated that knowledge of dengue was poor in around 38.6% (174/450) of respondents, moderate in 40.0% (180/450) and good in 21.4% (96/450) (Figure 1).
Assessment of Attitude of Respondents towards Dengue: The majority of the study cohort (389/450; 86.4%) considered that dengue is a serious disease, while just under one-third of students (138/450; 30.7%) had personal experience of a dengue infection. Exactly 80% of participants (360/450) said that there is a cure for dengue (Table 4).
Assessment of Practice of Respondents regarding Dengue: As may be seen from the preceding assessment of knowledge regarding dengue, four in every five respondents (366/450; 81.3%) know that standing water (contained in, for example, coolers, utensils, buckets and flower pots) provides a common breeding site for Aedes mosquitoes. In keeping with this awareness, most students suggested that preventing standing water from collecting in and around the domestic dwelling, by one means or another, is an important way to stop the spread of dengue. For instance, when asked about the frequency with which they clean water containers and empty ditches around their house, almost two-thirds (279/450; 62.0%) of participants did so once a week or more often, yet one-quarter (118/450; 26.2%) never undertook these mosquito prevention measures.
When asked what personal preventive measures they take to reduce the risk of mosquito bites, 63.6% (286/450) of students replied that they apply mosquito repellent, 84.7% (381/450) indicated that they wear long-sleeved garments, while just over half (250/450; 55.6%) of subjects advocated using All Out ® or other proprietary mosquito repellent at night (Table 5). In contrast, only around one-quarter of the cohort (108/450; 24%) slept under mosquito nets, with 14.4% (53/450) responding that they do not use any method to prevent mosquito bites.
Discussion
The results of this study indicate a general lack of knowledge of university students in Punjab towards dengue. A demonstrable understanding of the viral disease, its transmission by mosquitoes and its prevention was similar among students, irrespective of age, gender, place of residence, and, perhaps surprisingly, level and stream of academic study. The attitude of students reflects insufficient levels of seriousness and awareness regarding dengue. Of 450 respondents, only 21.4% demonstrated a good knowledge of dengue. The preventive measures taken by respondents were often not effective in - preventing dengue. A large proportion of subjects, 38.0%, reported that they do not regularly empty water-filled containers and ditches around their houses in order to prevent vector Aedes mosquitoes from breeding.
Our findings are in accord with those of two similar recent surveys conducted in Malaysia and Iran, the former a dengue-endemic country and the latter one in which potential vectors are becoming established and which infection is emerging [21,22]. In the Malaysian study, of 372 students and staff of a public university in Kuala Lumpur a major proportion of respondents had misconceptions about mosquito biting habits (83.8 %), seasonality of dengue epidemics (73.2 %) and mosquito breeding sites (70.3 %). It was advised that educational campaigns to promote preventive practices to combat dengue should focus on students, young staff members and those with lower level of education and income [21]. In the Iranian study, the cohort comprised a convenient sample of 30 international students of public health attending university in Tehran, all of whom were citizens of dengue-endemic nations. Despite inherent methodological flaws associated with the small sample size, the results suggested that international students did not have enough KAP regarding dengue [22].
Conclusion
This study suggests that as a way to reduce the threat of future outbreaks dengue awareness campaigns should target higher education students and other at-risk groups in urban areas of Punjab. In order to benefit the local community in which a person lives the findings indicate two priorities for urgent action: to increase their knowledge of effective mosquito control measures; and to raise their awareness of the need to take individual responsibility for dengue prevention. These action points may be applicable to all regions of India as well as being relevant to other dengue-endemic countries.
Acknowledgement
We would like to thank all participants for their completion of the questionnaire. We acknowledge the institutional ethics committee at Lovely Professional University for approval to perform the study. We are also grateful to members of faculty of the School of Pharmaceutical Sciences for their valuable suggestions in preparing the survey.
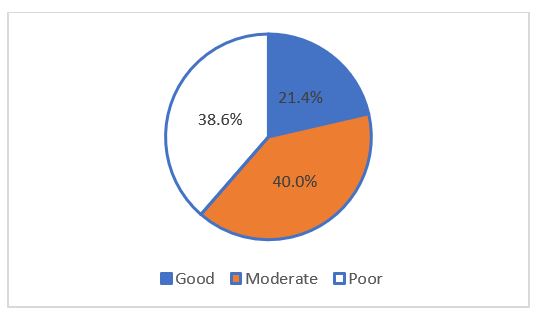
Figure 1: Survey respondents’ knowledge score regarding dengue.
|
Month |
Aug 2017 |
Sep 2017 |
Oct 2017 |
Nov 2017 |
|||||||||
|
Activity |
Day |
1st |
10th |
31st |
1st |
10th |
31st |
1st |
10th |
31st |
1st |
10th |
31st |
|
Review of literature |
|
|
|||||||||||
|
Design of experiment |
|
||||||||||||
|
Selection of sample |
|
||||||||||||
|
Questionnaire formulation |
|
||||||||||||
|
Pilot study |
|
||||||||||||
|
Conduction of survey on large scale |
|
|
|
|
|||||||||
|
Data compilation, report submission |
|
|
|
||||||||||
Table 1: Study work plan showing activity timelines.
|
Category |
Variable |
Frequency |
Percent |
|
Age (years) |
16-20 |
177 |
33.0 |
|
21-25 |
241 |
53.6 |
|
|
26-30 |
32 |
7.1 |
|
|
Gender |
Male |
267 |
59.3 |
|
Female |
183 |
40.7 |
|
|
Living status |
Rural area |
156 |
34.7 |
|
Urban area |
294 |
65.3 |
|
|
Study level |
Diploma |
80 |
17.8 |
|
Bachelors |
242 |
53.8 |
|
|
Masters |
105 |
23.3 |
|
|
PhD |
23 |
5.1 |
|
|
Study stream |
Engineering |
140 |
31.1 |
|
Applied Medical Sciences |
83 |
18.4 |
|
|
Business and Management |
114 |
25.3 |
|
|
Arts and Design |
39 |
8.7 |
|
|
Other |
74 |
16.7 |
Table 2: Major demographic characteristics of survey respondents.
|
Question |
Option |
Frequency |
Percent |
|
Which of the following diseases is/are transmitted by mosquitoes? |
- |
- |
- |
|
Wrong |
267 |
59.3 |
|
|
Right |
183 |
40.7 |
|
What are the most common symptom(s) of mosquito-borne diseases? |
- |
- |
- |
|
(a) Tiredness (b) Skin rashes (c) Joint pain (d) Headache (e) Fever (f) Muscle ache |
Wrong |
302 |
67.1 |
|
Right |
148 |
32.9 |
|
|
What are the complications of dengue infection? |
- |
- |
- |
|
(a) Shock (b) Low platelet count (c) Dehydration (d) Death |
Wrong |
115 |
25.6 |
|
Right |
335 |
74.4 |
|
|
Which of the following is/are NOT a mode of spread of dengue? |
- |
- |
- |
|
- |
- |
- |
|
Wrong |
302 |
67.1 |
|
|
Right |
148 |
32.9 |
|
|
Can dengue be transmitted by direct contact with another person? |
Wrong |
112 |
24.9 |
|
Right |
338 |
75.1 |
|
Identify the type/species of mosquitoes that transmit dengue: |
Wrong |
224 |
49.8 |
|
Right |
226 |
50.2 |
|
In a 24-hour period what is the most frequent dengue mosquito biting period? |
Wrong |
175 |
68.9 |
|
(a) Day time/morning (b) Night time/evening |
Right |
275 |
61.1 |
|
What are typical places in which mosquitoes breed? |
- |
- |
- |
|
Wrong |
306 |
68 |
|
Right |
144 |
32 |
|
|
Do mosquitoes breed in standing water? |
Wrong |
84 |
18.7 |
|
Right |
366 |
81.3 |
|
Dengue is most prevalent in which season of the year? |
- |
- |
- |
|
Wrong |
263 |
58.4 |
|
Right |
187 |
41.6 |
Table 3: Survey respondents’ knowledge regarding dengue.
|
Question |
Option |
Frequency |
Percent |
|
Dengue is a illness |
Serious |
389 |
86.4 |
|
Not serious |
39 |
8.7 |
|
|
Not sure |
22 |
4.9 |
|
|
Have you ever experienced dengue? |
Yes |
138 |
30.7 |
|
No |
312 |
69.3 |
|
|
Currently, is there any cure for dengue? |
Yes |
363 |
80.7 |
|
No |
60 |
13.3 |
|
|
Not sure |
27 |
6 |
|
|
Which of the following is beneficial for dengue patients? |
Taking plenty of rest |
152 |
33.8 |
|
Drinking plenty of water |
95 |
21.1 |
|
|
Eating fruit |
118 |
26.2 |
|
|
Antibiotics |
85 |
18.9 |
|
|
Is it possible to prevent/control? mosquitoes? |
Yes |
360 |
80 |
|
No |
49 |
10.9 |
|
|
Not sure |
41 |
9.1 |
|
|
Who is responsible for management of mosquito prevention/control? |
You |
78 |
17.3 |
|
Government |
38 |
8.4 |
|
|
Both |
333 |
74 |
|
|
No one |
1 |
2 |
|
|
Should communities actively participate in controlling vectors of mosquito-borne diseases? |
Agree |
359 |
79.8 |
|
Is controlling mosquito breeding places a good strategy to prevent dengue? |
Disagree |
47 |
10.4 |
|
Not sure |
44 |
9.8 |
|
|
Agree |
339 |
75.3 |
|
|
Disagree |
60 |
13.3 |
|
|
Not sure |
51 |
11.3 |
|
|
Have you attended any talk or workshop about prevention of dengue? that |
Yes |
201 |
44.7 |
|
No |
249 |
55.3 |
|
|
Would you wish to attend a talk or workshop relating to dengue prevention measures? |
Yes |
306 |
68 |
|
No |
144 |
32 |
Table 4: Survey respondents’ attitude towards dengue.
|
Question |
Option |
Frequency |
Percent |
|
Do you cover drinking water containers in your house? |
Yes |
396 |
88 |
|
No |
54 |
12 |
|
|
Do you use mosquito screen/mesh on windows and outside doors? |
Yes |
358 |
79.6 |
|
No |
92 |
20.4 |
|
|
Do you use any mosquito control aid during sleep at night? |
Mosquito repellent |
250 |
55.6 |
|
Mosquito net |
108 |
24 |
|
|
Insecticide spray |
14 |
3.1 |
|
|
Other |
13 |
2.9 |
|
|
Do not use any method |
53 |
14.4 |
|
|
Do you use larvicidal oil/kerosene in coolers/drains to kill mosquito larvae? |
Yes |
246 |
54.7 |
|
No |
204 |
45.3 |
|
|
Do you clean or empty flower pots/vases regularly? |
Yes |
350 |
77.8 |
|
No |
100 |
22.2 |
|
|
Do you turn containers upside down to avoid water collection in and around your house? |
Yes |
309 |
68.7 |
|
How frequently do you clean or empty water-filled containers and ditches around your house? |
No |
141 |
31.3 |
|
Always |
194 |
43.1 |
|
|
Once a week |
85 |
18.9 |
|
|
Once a month |
53 |
11.8 |
|
|
Never |
118 |
26.2 |
|
|
Do you cut down bushes in your yard or local park regularly to reduce mosquitoes? |
Yes |
310 |
68.9 |
|
No |
140 |
31.1 |
|
|
Do you apply mosquito repellent to exposed parts of your body? |
Yes |
286 |
63.6 |
|
No |
164 |
36.4 |
|
|
Do you wear long-sleeved shirts and long trousers to avoid mosquito bites? |
Yes |
381 |
84.7 |
|
No |
69 |
15.3 |
Table 5: Survey respondents’ practice regarding dengue prevention measures.
Citation: Prashar PK, Dutta S, Neha, Kumar B, Taylor-Robinson AW and Amarjeet Singh (2019) Knowledge, Attitude and Practices of University Students towards Prevention of Dengue in Northern India: A Questionnaire-Based Study. Emerg Infect Dis Diag J: EIDDJ-100002
