
Annals of Medical & Surgical Case Reports
Research Article
The Problem of Cognitive Impairments in Young Men with Epilepsy
Voitiuk A.* and Litovchenko T.
Department of Neurology and Child Neurology, KMAPE, Ukraine
*Corresponding author: Anna Voitiuk, Department of Neurology and Child Neurology, KMAPE, Ukraine, Tel: +380509081085; Email: a_vojtyuk@yahoo.com
Citation: Voitiuk A and Litovchenko T (2019) The Problem of Cognitive Impairments in Young Men with Epilepsy. Ann Med & Surg Case Rep: AMSCR-1000015.
Received date: 19 August, 2019; Accepted date: 26 August, 2019; Published date: 30 August, 2019
Abstract
Epilepsy is a chronic disease of the central system with a wide range of neuropsychiatric disorders. Cognitive disorders are quite common with this disease and significantly reduce the quality of life of patients and their families. In approximately 35% of patients, despite treatment, various impairments of memory, attention and bradyphrenia persist in the interictal period. Causes of cognitive impairment in patients with epilepsy can be directly the underlying factor of epilepsy (genetic disease, structural brain defect, etc.), epileptic seizures, interictal epileptiform activity, side effects of antiepileptic drugs (AEDs). Modern neurophysiological and neuroimaging diagnostic methods allow us to identify new features of the course and progression of dysfunctions of higher nervous activity in epilepsy.
Keywords: Antiepileptic therapy; Cognitive impairments in young men; Epilepsy; Pathogenesis of disorders
Introduction
Epilepsy is one of the most common severe diseases of the nervous system, which occurs 10 times more often than multiple sclerosis and 100 times more often than motor diseases. Epilepsy takes third place in frequency after dementia and strokes [1-3].
According to the consensus of the International League against epilepsy (International League Against Epilepsy, ILAE) and International Bureau for epilepsy (International Bureau for Epilepsy, IBE), epilepsy is a disease of the brain defined by any of the following conditions:
Epilepsy is considered to be resolved for individuals who had an age-dependent epilepsy syndrome but are now past the applicable age or those who have remained seizure-free for the last 10 years, with no seizure medicines for the last 5 years [4].
The problem of epilepsy attracts the attention of neurologists and psychiatrists around the world because of its widespread and great social significance. The prevalence of this disease in developed countries is 5-10 cases per 1,000 populations. According to the results of population studies conducted in developed countries, the incidence of epilepsy ranges from 0.28 to 0.53 per 1,000 populations. The prevalence of the disease varies from 0.96 to 10 cases per 1,000 populations in the CIS countries. In addition, the average incidence in men (53.7 per 100,000) is slightly higher than in women (46.3 per 100,000) [5].
Materials and Methods
There are discrepancies between the prevalence and incidence of epilepsy in Europe and Ukraine, as well as the heterogeneity of the prevalence of epilepsy in different regions of Ukraine. In Ukraine, an average of 50-73 people per 100,000 people suffer from epilepsy. In addition, this disease has a high level of disability [6].
Epilepsy is a chronic brain disease characterized by repeated unprovoked attacks of impaired motor, sensory, autonomic, cognitive and mental functions resulting from excessive neural discharges. This disease is one of the oldest recognizable neurological diseases in the world and is characterized by the wide distribution in the clinical picture of various neuropsychic disorders, which are one of the most important components of the clinical picture of the disease and significantly affect the quality of life and social adaptation. The leading place among all violations belongs to cognitive impairment [7]
Cognitive mental functions carry out the process of rational cognition of the world and purposeful interaction with it. They are formed as a result of the integrative activity of the brain, providing the person’s ability to receive, analyse, memorize information, share it, and also develop and implement an action program. Cognitive functions include memory, gnosis, speech, praxis, and intelligence [8]. Their disorders are the most common comorbid disorders in patients with epilepsy.
Cognitive impairments are a clinical manifestation of epilepsy, which are most correlated with the volume of affected brain tissue and determines the quality of life of patients. They are the best indicator of the dynamics of the disease and the effectiveness of therapy. A specific feature of the neuropsychological profile of cognitive impairment in epilepsy is the predominance of regulatory and neurodynamic disorders associated with dysfunction of the frontal lobes and deep parts of the brain. In some cases, these disorders can disable the patient more than epileptic seizures [9].
Various factors play an important role in the pathogenesis of cognitive impairments: the etiology of the disease, the type and frequency of epileptic seizures, interictal epileptiform activity on the electroencephalogram (EEG), premorbid factors, the use of certain antiepileptic drugs (AEDs), psychosocial factors that lead to aggravation of seizures (Figure 1).
One of the factors that have a negative effect on cognitive function is the etiology of epilepsy. The causative factors can be acquired diseases (traumatic brain injury, stroke, consequences of neuroinfection, etc.) and genetic diseases (Drave’s, Rett’s syndromes, tuberous sclerosis, etc.) [10]. At the international epileptological congress in Barcelona in 2017, the term “epileptic encephalopathy” was introduced, which means that with encephalopathies of development, cognitive and behavioural disorders are caused by the disease itself, and their course does not depend on the treatment of AEDs [11].
Various characteristics of epileptic seizures act as predictors of intellectual deficiency. All researchers agree that the age of the onset of seizures up to 3-5 years of life correlates with a poor prognosis regarding intellectual status [12]. The duration of the history of epilepsy affects cognitive function at a sufficiently high frequency and severity of seizures. In the genesis of cognitive impairment for any type of seizure, glutamate-mediated excitotoxic effects that cause damage and death of brain neurons, especially in the structure of the hippocampus, are currently of particular importance [13].
According to various studies, there is a clear relationship between cognitive impairments and the localization of the paroxysmal focus. For example, in temporal epilepsy, the cognitive sphere suffers the most when the focus is located in the mediobasal portions of the temporal lobe. The weakening of various functions (for example, memory, verbal and spatial functions, etc.) depends on the dominance of the hemisphere [14].
Cognitive impairments are closely related to the phenomenon of brain aging. The main causes of the development of epilepsy are premorbid insolvency plus cerebrovascular pathology, stroke, trauma and neurodegenerative diseases [15].
Recently, much attention has been paid to the impact on cognitive status of not only the parasites themselves, but also interictal epileptiform activity on the EEG. The causal relationship between the interictal discharges on the EEG and cognitive deficit is confirmed by the fact that with the effective treatment of seizures and normalization of the EEG, the intellectual status of patients is dramatically improved. Syndromes of acquired disorders of higher mental functions associated with epileptic activity on the EEG in the absence of clinical attacks indicate the possibility of an effect on the cognitive functions of the epileptic activity itself. In experiments, it was shown that during subclinical generalized and focal epileptic discharges on EEG in 50% of patients, the implementation of psychometric tests slows down.
Epileptic discharges and cognitive functions have bidirectional relationships: not only epileptiform activity (Figure 2) affects cognitive status, but mental stress can suppress or cause epileptic discharges. It is known that epileptic seizures can be triggered by reading, counting, talking, certain thoughts, mental stress, etc. Linguistic stresses cause spike activity more often in the left hemisphere of the brain, tasks for spatial praxis in the right [16].
According to the latest recommendations of the ILAE, epilepsy can be considered permitted if the patient has not had seizures for 10 years, and for the last 5 years he has not taken AEDs, and also if the patient has passed the age at which age- dependent forms of epilepsy appear [4].
Currently, it is shown that almost all AEDs can affect cognitive functions, affective sphere and behaviour of patients. Phenobarbital has one of the pronounced negative effects; dose-dependent effects on attention, short-term memory, intelligence and reaction rate, and, most important, on speech skills, are described. A side effect of carbamazepine is associated with its metabolite - carbamazepine epoxide. There is evidence of dose-dependent cognitive impairments when using carbamazepine, as confirmed by Jokeit [17], which shows a negative dependence of temporal region activation (according to fMRI) in patients with temporal lobe epilepsy and serum carbamazepine levels.
Ethosuximide also has a negative effect. The reaction rate, thought processes, various indicators of attention (including switching attention) and prolonged auditory concentration are directly caused by the action of the drug itself. One of the rare, but most serious complications is the development of psychosis. According to the literature, ethosuximide can cause psychosis, suicidal thoughts and symptoms of manic disorder [18,19].
According to the results of some studies, valproic acid preparations do not cause cognitive impairment, there are no significant deviations in the memory of the reaction rate and thinking [18]. Another drug with a good cognitive profile is lamotrigine. In a comparative placebo-controlled study [20], lamotrigine showed good results of concentration and mental activity in patients with epilepsy.
The choice of topiramate in the treatment of epilepsy in some cases may be limited due to its effect on cognitive function. When studying the effects of topiramate in epilepsy, a slowdown in thinking, drowsiness, fatigue, and a decrease in concentration were recorded [21].
According to the report of the ILAE working group, levetiracetam has a positive effect on cognitive function, but it negatively affects behaviour. Apparently, levetiracetam does not have a negative effect on the cognitive functions, but there are insufficient data [22].
Results
For clinical trials, it was selected men aged 18-44 years with epilepsy without topical somatic diseases.
An ethical commission was convened to conduct this study. After reviewing the research data and discussing all issues, the ethics committee approved the study.
The purpose of this study is to determine the level of cognitive impairment in young men suffering from epilepsy, and to assess their psycho-emotional state. The study was based on an analysis of clinical symptoms and instrumental research data, and also included neuropsychological testing using the MMSE (Mini-Mental State Examination) scale and the STAI (State-Trait Anxiety Inventory) scale. EEG, CT, MRI were used as screening methods.
All 40 patients aged 18-44 years noted anxiety, concern about their health, and a decrease in self-esteem. Most patients (28 out of 40 patients) complained of a decrease in cognitive functions-short-term and long-term memory, attention. Assessment of indicators of personal and situational anxiety was carried out according to the STAI scale (Table 1).
Cognitive functions were evaluated on the MMSE (Mini-mental Score) scale. Analysis of test data from 40 patients (100%) showed that 12 (30%) of them had mild cognitive impairments. Moderate cognitive impairments were observed in 22 patients (55%). Mild and moderate dementia were observed in 4 (10%) and 2 (5%) patients respectively (Figure 3).
The first factor that has a negative impact on cognitive function is the etiology of epilepsy. In patients with symptomatic epilepsy, the intellect suffers more often than in patients with cryptogenic epilepsy (Table 2).
The next factor is the role of epileptic seizures in the development of cognitive impairments. Continuing epileptic seizures can cause persistent and progressive changes in neural connections, and in some cases brain structures. Patients with generalized tonic-clonic seizures showed worse rates of intellectual and neuropsychological testing. In patients with generalized and combined seizures, the indicators are worse than in patients with focal seizures.
Also in the development of cognitive impairments are influenced by interictal epileptiform activity. Epileptiform activity alone can contribute to severe cognitive and behavioural disorders, except and beyond those that are expected in the disease itself and that may deteriorate over time [Figure 4].
Epilepsy is a disease that requires long-term (at least 3 years after the cessation of attacks) therapy. The effectiveness of AEDs is due to their mechanism of action (pharmacodynamics). However, the nature of the side effects is also determined to some extent by the mechanism of action of AEDs. This is especially true for cognitive impairments that occur during therapy, since, by suppressing epileptiform activity, AEDs affect the areas of the brain involved in the processes of memory, learning, and regulation of emotional reactions [22].
Antiepileptic therapy was given to these patients. Valpro?om (valproic acid preparation) was chosen as the main drug for 4 patients (10%), 16 people (40%) took carbamazepine, lamotrigine was prescribed to 12 patients (30%), and levetiracetam 8 people (20%) (Figure 5). Patients with epilepsy who took valprocom and carbamazepine showed an improvement in mood. Patients who received lamotrigine noted an improvement in attention and behaviour. Patients who were prescribed levetiracetam did not notice any changes other than worsening behaviour.
Discussion
Thus, the study of disorders of higher nervous activity in epilepsy remains an urgent problem of modern neurology. The occurrence of cognitive impairment is an integral part of the course of epilepsy and affects the general condition of the patient at different stages of the disease.
Conclusion
Currently, the discussion continues on the role of each factor in the development of cognitive impairment in epilepsy, attempts are made to find the optimal ratio of doses of AEDs, which would not have a pronounced effect on higher nervous activity. Socialization of patients and assistance in cognitive impairment remain an important task.
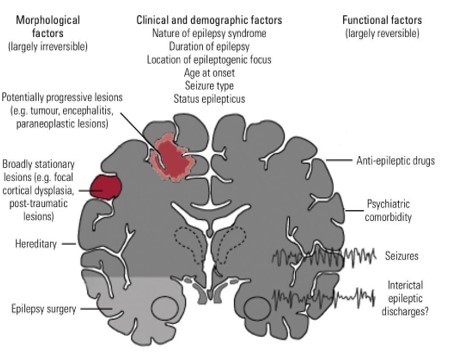
Figure 1: Factors affecting cognitive function in epilepsy.
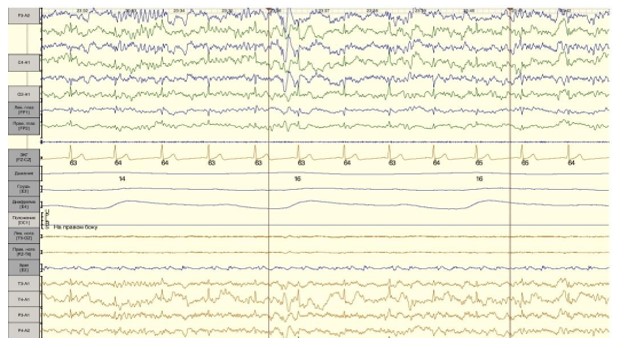
Figure 2: Patient T., male, 39 y.o. A fragment of the EEG.
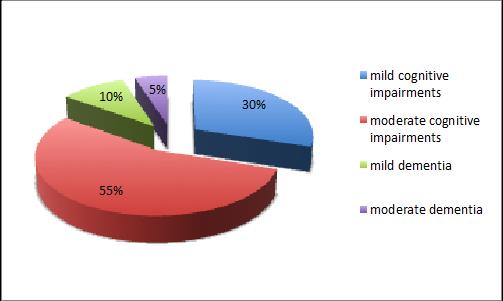
Figure 3: An assessment of cognitive functions on the MMSE scale.
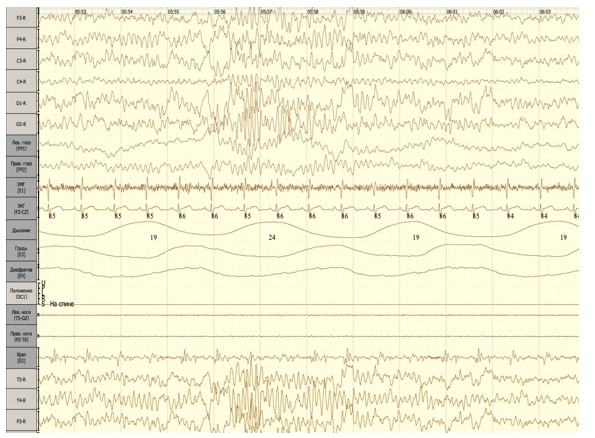
Figure 4: Patient S., male, 35 y.o. A fragment of EEG.
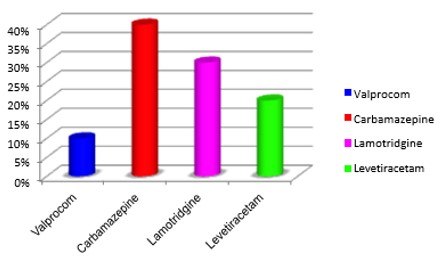
Figure 5: Antiepileptic therapy.
|
Age |
Score |
|
18-30 |
33.7 ± 0.2 |
|
31-40 |
46.2 ± 0.3 |
|
41-44 |
41.5 ± 0.4 |
|
Note:*differences significant p>0,005. |
|
Table 1: An assessment of personal and situational anxiety indicators on the STAI scale.
|
Form of epilepsy |
Memory function violation
|
Attention disorder |
Speech disorder |
Thinking disorder |
|
Symptomatic (total 25 people; 62.5%) |
15 (60%) |
12 (48%) |
4 (16%) |
18 (72%) |
|
Cryptogenic (total 11 people; 27.5%) |
9 (82%) |
7 (64%) |
2 (18%) |
7 (64%) |
|
Idiopathic (only 4 people; 10%) |
3 (75%) |
2 (50%) |
- |
2 (50%) |
Table 2: Indicators of the cognitive sphere depending on the form of epilepsy.
Citation: Voitiuk A and Litovchenko T (2019) The Problem of Cognitive Impairments in Young Men with Epilepsy. Ann Med & Surg Case Rep: AMSCR-1000015.
