
Annals of Medical & Surgical Case Reports
Research Article
Knowledge, Attitude and Practice of Breast Self-Examination Among Sudanese Females Attended to Omdurman Maternity Hospital in Sudan
Kunna A1, Rawia M Osman4, Khairy S Ismail2, Hassan A Elkheir3*, Suad Enour2 and Umbeli Taha2 Khairy S5
1Department of Obstetrics and gynecology, University of Bahri, Sudan
2Department of Obstetrics and gynecology, Omdorman Islamic university, Sudan
3Omdorman Maternity Hospital, Central laboratories, Khartoum, Sudan
4Ministry of Health, Sudan
5University of Bahri, Sudan
*Corresponding author: Akram Elkhier Hassan, Omdorman Maternity Hospital, Central laboratories, Khartoum, Sudan, Tel: +249966552833546; Email: akramalk@yahoo.com
Citation: Kunna A, Ismail KS, Enour S, Taha U, Elkheir HA, et al. (2019) Knowledge, Attitude and Practice of Breast Self-Examination Among Sudanese Females Attended to Omdurman Maternity Hospital in Sudan. Ann Med & Surg Case Rep: AMSCR-1000020.
Received date: 16 September, 2019; Accepted date: 21 September, 2019; Published date: 30 September, 2019
Abstract
Background: Breast self-examination is expected to serve early detection and accordingly better management in countries with insufficient health services settings.
Objectives: To assess the knowledge, attitude and practice of breast self-examination (BSE) among Sudanese females attended to Omdurman Maternity Hospital (OMH).
Method: This is a prospective cross-sectional hospital-based study recruited 389 females attended to Gynecological and Obstetric departments at Omdurman Maternity Hospital during April 2017- to Sept. 2017. Variables of the study included demographic data, knowledge about breast cancer and breast self-examination, attitude and practice towards breast self-examination, factors affect their knowledge and practice and source of knowledge. Data was collected by using pre-designed questionnaire, then analyzed by using Statistical package for social science (SPSS). Chi-square test was used for cross-tabulation at p value (0.05) and 95% confidence interval.
Results: Out of 389 females, the age group of 20-30 years was the commonest 224 (57.6%), while 168 (43.2%) and 162(43.2%) received secondary school and university education respectively and 319 (82%) reside in urban areas. Family history of breast cancer was reported in 100 (25.7%). The overall score of knowledge and attitude about breast self-examination were found moderate (54.6% and 59.8% respectively); among which knowledge and attitude were most commonly poor regarding time of performing the BSE and phobia of detecting the cancer (39.6% and 42.2% respectively). The study also revealedVIpoor performance towards BSE (34.6%). Knowledge about BSE found significantly associated with family history of breast cancer, age and education (P< 0.05). Practicing BSE found significantly associated with higher level of education, receiving training or counseling and history of other breast disease (P<0.05). Media and heath cadres are the commonest source of knowledge about breast self-examination (41.5% and 21.3% respectively).
Conclusion: The current findings have revealed unsatisfying levels of knowledge and attitude and poor practice about breast self-examination among Sudanese female attended to OMH.
Keywords: Breast cancer; Maternity; Breast self-examination (BSE); Sudan; World Health Organization (WHO)
Introduction
In 2008, it was estimated that the prevalence of breast cancer in women aged 15 years and over in Sub-Saharan Africa is 23.5 per 100,000 women [1]. Breast cancer has been identified as a major public health problem in both developed and developing nations because of its high incidence-prevalence, the over-burdened health system and direct medical expenditure [2]. Global statistics shows that the annual incidence of breast cancer is increasing and this is occurring more rapidly in countries with a low incidence rate of breast cancer. Findings from [3] documented that the incidence of breast cancer in Nigeria has risen significantly with incidence in 2009-2010 at 54.3 per 100 000, thereby representing a hundred percent increase in the last decade. Some cases have been reported among women aged below 30 years in Nigeria. This is supported by the literature showing a rise in breast cancer incidence rates in Sub-Saharan Africa [4].
Breast self-breast examination (BSE) is culturally acceptable, religious friendly and attracts no cost. Women's knowledge and beliefs about breast cancer and its management may contribute significantly to medical help-seeking behaviors. This study aimed to assess knowledge and beliefs of BSE among market women. Early detection of breast cancer plays an important role in decreasing its morbidity and mortality [1]. This study therefore examines the factors influencing breast self-examination (BSE) awareness and practices among women in Ogun state, Western Nigeria. Breast cancer has increasingly become an issue of public health importance. In the year 2000, there were 10 million new cases of cancer and 6 million cancer deaths worldwide [5].
Women’s Knowledge, attitude and practice towards breast-self-examination: The high incidence of breast cancer necessitates the need for early detection because this would increase the treatment options available to affected women and thereby improve survival rates [6]. Some studies have shown that in most of the developing nations and resource constraint settings, breast cancer is diagnosed in advanced stages of the disease when compared with developed nations and thus has a poor outcome and high fatality rate [7].
Screening for early detection and diagnosis of diseases and health conditions is an important public health principle [8]. Breast self-examination (BSE) is a check-up that a woman does by herself at home to look for changes or problems affecting the breast tissue. BSE is still recommended as a general approach to increasing breast health awareness and thus potentially allow for early detection of any anomalies because it is free, painless and easy to practice [9]. The American Cancer Society [10] also recommends that women, starting from the age of 20 years should be educated on the pros and cons of performing a monthly BSE. For women to present early to hospital they need to be "breast aware"; they must be able to recognize symptoms of breast cancer [11].
There are reports suggesting that factors related to women's knowledge and beliefs about breast cancer and its management may contribute significantly to medical help-seeking behaviors [12]. Recent studies in Senegal, Angola and Nigeria [13] revealed a low level of awareness and knowledge on breast cancer risk factors and its early warning signs. Lack of understanding of the risk factors associated with breast cancer discourages people from seeking early intervention or even to admit that symptoms they may be experiencing are related to breast cancer. As such there is need for a study to assess knowledge and beliefs about breast examination BSE and risk factors among women in our communities. This study therefore aimed to assess the knowledge and beliefs of breast self-examination and breast cancer among market women in densely populated markets in Ibadan, Oyo State, Nigeria.
Problem Statement: Breast cancer (BC) is the top cancer in women, both in the developed and in the developing world [14]. Many case of breast cancer among females in Sudan discovered at late stage and develop to more serious stage or end with mortality. Some studies in Sudan have indicated that, death due to breast cancer among Sudanese ladies is very common in Sudan [15].
Justification: Breast self-examination is one of the main methods of early detection of breast cancer among females as well as it is a simple method with higher compliance since it saves women’s privacy. Early detection enables good management and accordingly better outcome. Although there are great efforts to raise community attention towards breast self-examination, there is a need for more sustainable and extended evaluation of breast cancer and self-examination among Sudanese ladies. Also, there is poor knowledge among females in Sudan about breast self-examination.
Materials and Methods
Study Design: This is prospective cross-sectional hospital-based study.
Study Area: This study was conducted in the refer clinic at Omdurman Maternity Hospital, which is a biggest breast center in Sudan. It is established in 1957 and it represents the major maternity hospital in Sudan, and it offers emergency and elective obstetrics and gynecology services during the 24 hours. It serves patients from Khartoum state and other different parts of Sudan with estimated rate of 60-80 vaginal deliveries per day, 30-50 elective and emergency caesarean sections.Out patients receive about 250-300 per day, (gynecological cases: about 50-75, private: about 30-40, obstetric cases about 150-200). The capacity of Omdurman maternity Hospital is 200 beds. The labor room consists of the following: outpatient, low risk, high risk, high dependency room (zero room).
Study period: This study was conducted from April 2017- to Sept. 2017.
Study Populations: Sudanese females attended to refer clinic at Omdurman Maternity Hospital.
Inclusion criteria: Females who attended to Gynecological and Obstetric refer clinic during the study period.
Exclusion criteria: Females who refused to participate.
Sample size: The sample size was calculated by using Colvin’s formula, considering that, the total patient’s attendance in gynecological and Obstetric refer clinic during the study period is 14400:
n=N/1+N(e2)
n=N/1+N(e2)
Where:
n = required sample size
N = total population during six months (14400)
E = margin of error at 95% confidence interval (0.05)
n=14400/1+14400(0.0025) = 389
Data Collection
Data collection Tools: Data was collected by using structured designed questionnaire to assess the knowledge, attitude and practice of BSE among females attended to ANC clinic at Omdurman Maternity Hospital.
Data collection Technique: By the predesigned questionnaire, the questionnaire was managed by the author. Patients were selected randomly by choosing the first patients met in refer clinic until satisfying the desired sample size.
Data processing and analysis: Data analysis was accomplished by using the statistical package for social sciences (SPSS, version. 23). Cross-tabulation was calculated by chi-square test at p value 0.05 and 95% confidence interval.
Study variables: Variables in the study included socio-demographic data, questions on knowledge, attitude and practice about breast self-examination in addition to source of information.
Ethical Considerations
Result
Discussion
Breast cancer is major public health concern in both developing and developed countries. The WHO has in its latest report on the global situation of cancer, indicated 7600 fatalities in 2014 among females in the Sudan because of cancer, 23.9% of them because of breast cancer [16]. Breast self-examination is expected to serve early detection and accordingly better management in countries with insufficient health services settings.
Demographic characteristics: Demographic characteristics of females participated in the current study indicated that, most of them were in the age of 20-30 years or 31-40 years (57.6% and 32.1% respectively), had either secondary or university educational degrees (43.2% and 41.6% respectively). the commonest occupation among participants was housewife which reported in more than half of participants (57.6%) as well as vast great majority of them were married (72.8%) and reside in urban areas (82 %).
Overall Score of Knowledge: The current findings have revealed that, the overall score of knowledge about breast self-examination among Sudanese female attended to OMH was moderate(54.6%), suggesting that, females have unsatisfying level of knowledge, although the majority of them reported to be aware about the terms “breast cancer’ (96.7%), as well as most of them knew what BSE means and its importance in early detection of breast cancer (70.4% and 71.2% respectively); they showed poor knowledge regarding some criteria associated with the BSE procedure such as knowing that BSE is performed monthly (39.6%), Know the 3 positions to perform BSE (23.4%) and time of doing the BSE during the month (30.8%).
A study by in Sudan among female medical students reported better knowledge, the study showed that, most respondents (86%) were aware of BSE [17]. But, most studies conducted among public females in Developing countries reported poor knowledge as Recent studies in Senegal, Angola and Nigeria revealed a low level of awareness and knowledge on breast cancer risk factors and its early warning signs [12, 17,18]. A study in Nigeria by reported insufficient awareness towards breast self-examination and called for encouraging females for examination. Findings of the same study have indicated that, some females (30%) knew the different methods for screening for breast cancer, however most of them (56%) knew that breast-self-examination should be performed monthly [19].
Difference in studied areas and type of populations in Sudan might show some discrepancies in level of awareness towards breast cancer. Yet, some facts might show beyond discrepancy in studies, as shown by in the Sudan International Conference on Breast Cancer in 2011 who indicated that, breast cancer in Sudanese women is in the rise and 80% - 85% of breast cancer patients presented with late advanced disease [20].
The main source of knowledge about BSE is TV/ radio (41.2%), while there is poor participation from health providers, educational prints and websites in educating females about BSE (13.1%, 11.3% and 7.7%). The study of and colleagues at in Omdurman locality, agrees with our findings in regard to predomination of media as the main source of information about breast cancer and self-examination, they found that, women were received general information about breast cancer mainly from the media (73.9%) [21]. Even though among female medical student’s media in Sudan is considered as the main source of knowledge, and this was illustrated by who assessed the practice of breast self-examination in three Sudanese governmental universities and revealed that, mass media such as Newspaper, television and radio were the major source of information while information conducted by health workers was the least [22].
Attitude: Females in the current study also unsatisfying level of attitude towards BSE; they showed moderate overall score (59.8%). Their attitude was mostly negative towards phobia of detecting the cancer (42.2%), while they showed better attitude towards importance of screening (65.8%) and being motivated by publicity (67.6%) and more than half of them believe that BSE is ungraceful practice. An interventional study by reported better attitude towards BSE among women at Wad Nubaui-Omdurman (93.2%) [23]. A Malaysian study by agrees with our findings in regard to fear of detecting the breast cancer, they reported that, 38.5% of women surveyed does not worry to detect breast cancer [24].
Fear of detecting the breast cancer was reported less frequently in South Africa, they found that, about 28.5% agreed that fear of detecting breast cancer would make them not practice BSE, while more than 50% strongly disagreed with this statement [1].
India reviewed that, fear of detecting the disease is one of the main determinants that negatively impact early detection of breast cancer [25,26].
Practice: Assessing some criteria of practice about BSE among females showed poor performance (34.6%); only few of them found do BSE (23.4%); out of them (60.4%) do the self-examination in proper time (monthly); and they represented (14.1%) out of total participants. Few of females in the current study encourage friends to do the examination (28.3%). When the other females were inquired about the cause of not doing the self-examination, majority of them justified that; “it is hard to remember”(88.9%), while few mentioned that it takes too much time (6.7%) or feeling no privacy in doing the examination (4.4%) and reported proportionally better-but still unsatisfying-performance towards BSE among women at they found that, (53.6%) had ever performed BSE the main cause is lack of knowledge [23].
Practicing breast self-examination was found less frequent among women reside in rural areas in among females in India that reported by they found that, only 18% of the females had ever checked their breast and 5% practiced it regularly [25]. The Malaysian study by reported that, practicing BSE is not done by 70.5% of women due to lack of knowledge about the method of the examination [24].
Factors associated with practicing BSE: Practicing BSE found significantly associated with higher level of education; among illiterates no females reported to practice BSE, while it was practiced by 9.1% of females with basic schooling, 11.9% of females who were secondary school graduates, 38.9% of university graduates and 50% of postgraduate’s females (P = 0.000). This agrees with the findings of who concluded that, there was a statistically significant relationship between educational level and knowledge on how to perform BSE (p<0.0001) [1]. History of other breast disease revealed a significant association with practicing BSE; 41.7% of females with positive history of other breast disease, did BSE versus 22.2% of females with no history of other breast disease (P = 0.029).
Receiving training or counseling about methods of self-examination found significantly motivate female to do BSE when compared to those who didn’t receive any training or counseling; 65% of females who received training or counseling (65% vs. 21.1% respectively, P = 0.000).
Unexpectedly, family history of breast cancer found negatively impact doing BSE, and the association was revealed significant; only 36.3% of female with positive family history of breast cancer did the BSE versus 63.7% of females without family history of breast cancer (P = 0.008). This might be due to developing phobia from BSE among those who experienced breast cancer in the family, and such justification suggest poor attitude towards doctor counseling and awareness about the benefit of early detection. Many previous studies reported similar findings showing that, variables including age, level of education, personal history of breast problems, and family history of BC are not significant in BSE practice [21], and consistent findings were reported. A compatible findingwas shown by who reported that, age and breast cancer in the family variables were significantly associated with BSE practice.
Factors impacts Hearing about BSE and fear of detecting the breast cancer: Fearing of detecting the breast cancer found significantly impacted by level of education, family history of breast cancer and receiving training counseling about method of BSE but not affected by history of other breast disease (P = 0.000, 0.004, 0.004 and 0.335 respectively). Females with low education reported some confusion since most of them were not sure whether they afraid of detecting breast cancer or not, while females with university education or postgraduates showed better positive attitude by denying their fear of detecting breast cancer (61.4% and 75% respectively, P= 0.000). On the other hand, females who received training about methods of BSE found significant more afraid of detecting breast cancer (60%) while those who didn’t receive any training didn’t seem afraid (P = 0.004).
Those with positive family history of breast cancer were significantly more afraid of detecting breast cancer when compared to those without history of breast cancer (40% and 23.5% respectively, P = 0.004). Hearing about BSE found significantly associated with family history of breast cancer and age (0.019 and 0.020 respectively), while it was not impacted by history of other breast disease (P = 0.153). On the other hand, education found significantly impact hearing about breast cancer (0.004).
Females with family history of breast cancer were significantly more likely to hear about the term BSE when compared to those without family history of breast cancer (79% versus 67.5% respectively, P = 0.019). Females with age under 20 years less likely to hear about BSE (only 22.2%) while females in age exceeding 50 years found significantly more likely to hear about BSE (87.5%, P=0.020).
This agrees with a study from rural who found that, knowledge increased with increase in age [27]. While the study of colleagues reported disagreeing results showing that, age of the women had a negative correlation with knowledge [25].
Hearing about breast cancer found significantly higher among better educated females when compared to those with illiteracy or basic schooling (99.4% university and 100%postgraduates versus 85.7% illiterates and 88.6% basic school graduates, P=0.004). Awareness of BSE was found to be significantly associated with age and educational attainment. Positive impact of education on knowledge about BSE have been revealed in many other studies reporting that, women with higher level of education had better knowledge regarding breast cancer and BSE than women with low education status [28].
Impact of education and occupation: Source of information found significantly associated with media (TV & Radio) irrespective of occupation, while health cadres most feed housewives and employees (44.1% and 27.1% respectively, P=0.011). Females with limited education (illiterates and basic school) tend to receive information from family or friends, while females with secondary school, university or postgraduates tend to depend on TV and radio in receiving information about BSE.
Conclusion
The current findings have revealed unsatisfying levels of knowledge and attitude about breast self-examination among Sudanese female attended to OMH, although the majority were aware about breast cancer. Practicing breast self-examination was found to be poor, most of them justified that by not remembering the examination.
Practicing BSE found significantly associated with higher level of education, receiving training or counseling and history of other breast disease, while family history of breast cancer found negatively impact doing BSE. Fearing of detecting the breast cancer found significantly impacted by level of education, family history of breast cancer and receiving training counseling about method of BSE. Knowledge about BSE found significantly associated with family history of breast cancer, age and education but not impacted by history of other breast disease.
Recommendation
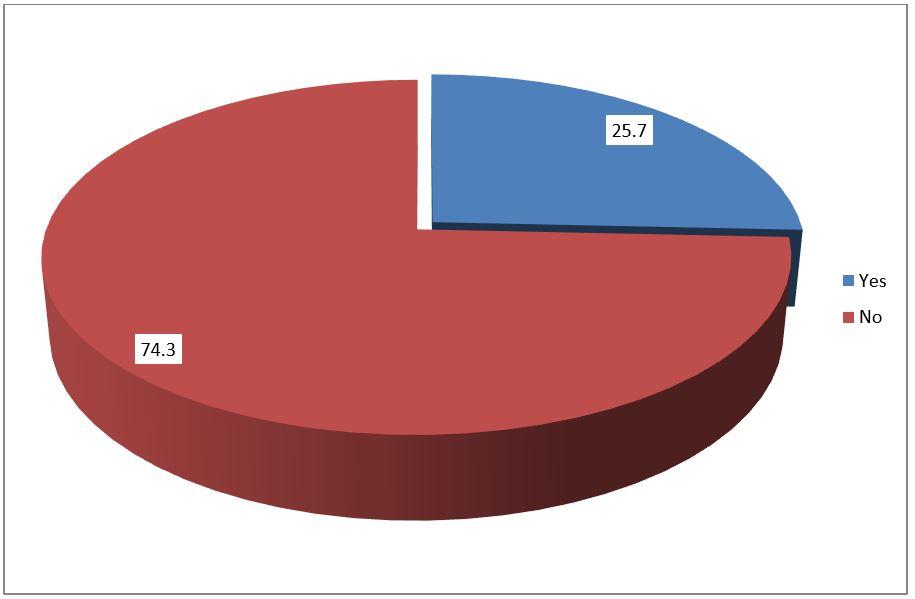
Figure 1: Family history of breast cancer among Sudanese females attended to OMH.
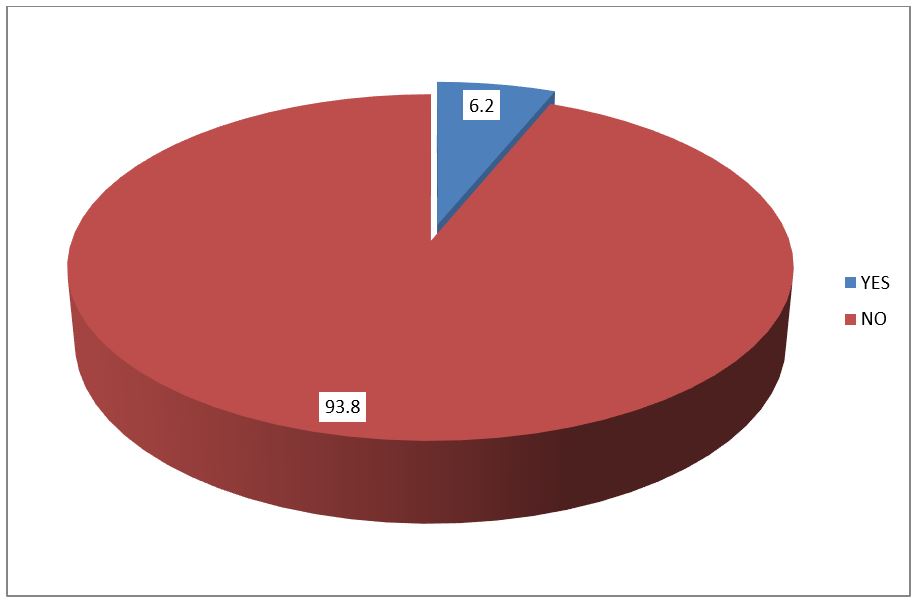
Figure 2: History of breast disease among Sudanese females attended to OMH.
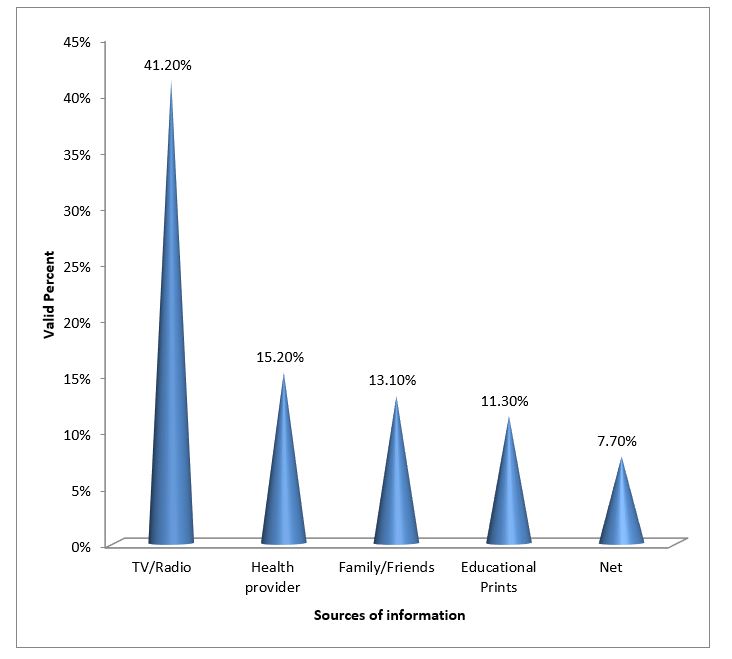
Figure 3: Sources of information about BSE among Sudanese females attended to OMH.
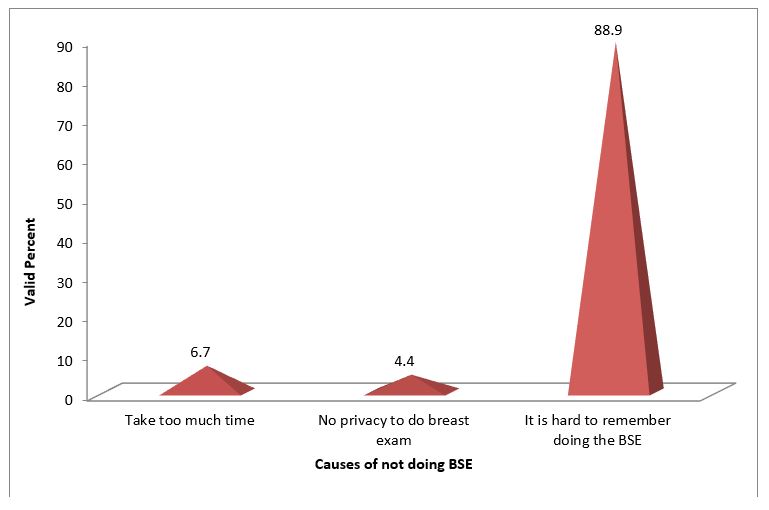
Figure 4: Causes of not doing BSEas reported by Sudanese females attended to OMH.
|
Demographics |
Frequency |
Percent |
|
Age group (years)0-+/- |
||
|
<20 |
9 |
2.3% |
|
20-30 |
224 |
57.6% |
|
31-40 |
125 |
32.1% |
|
41-50 |
23 |
5.9% |
|
>51 |
8 |
2.1% |
|
Education |
||
|
Illiterate |
7 |
1.8% |
|
Basic |
44 |
11.3% |
|
Secondary |
168 |
43.2% |
|
University |
162 |
41.6% |
|
Postgraduates |
8 |
2.1% |
|
Occupation |
||
|
Student |
26 |
6.7% |
|
House Wife |
224 |
57.6% |
|
Worker |
59 |
15.2% |
|
Employee |
70 |
18% |
|
Others |
10 |
2.6% |
|
Marital Status |
||
|
Single |
73 |
18.8% |
|
Married |
283 |
72.8% |
|
Divorced |
30 |
7.7% |
|
Widow |
3 |
0.8% |
|
Residence |
||
|
Urban |
319 |
82% |
|
Rural |
70 |
18% |
Table 1: Demographic characteristics of Sudanese females assessed about BSE at OMH.
|
Knowledge |
Frequency |
Percent |
|
Hearing About Breast Cancer |
376 |
96.7% |
|
Ever heard of BSE |
274 |
70.4% |
|
Know BSE should be performed monthly |
154 |
39.6% |
|
Know the 3 positions to perform BSE |
91 |
23.4% |
|
Know what to look for while performing BSE |
196 |
50.4% |
|
Know BSE is important in the early detection of breast cancer |
277 |
71.2% |
|
Time of doing the BSE |
120 |
30.8% |
|
Overall Score Of Knowledge (%) |
- |
54.6% |
Table 2: Knowledge about BSE among Sudanese females attended to OMH.
|
Attitude |
Frequency |
Percent |
|
Fear of detecting breast cancer |
||
|
Agree |
108 |
27.8% |
|
Disagree |
164 |
42.2% |
|
Not Sure |
117 |
30.1% |
|
Screening for abnormality of BSE is important and useful |
||
|
Agree |
256 |
65.8% |
|
Disagree |
28 |
7.2% |
|
Not Sure |
105 |
27% |
|
Being motivated by publicity or campaign about BSE |
||
|
Agree |
263 |
67.60% |
|
Disagree |
84 |
21.60% |
|
Not Sure |
42 |
10.80% |
|
BSE is ungraceful practice |
||
|
Agree |
18 |
4.60% |
|
Disagree |
247 |
63.5%` |
|
Not Sure |
124 |
31.90% |
Table 3: Attitude towards breast cancer and BSE among Sudanese females attended to OMH.
|
Practice |
Frequency |
Percent |
|
The ability to self-detection of breast cancer |
||
|
Agree |
217 |
55.8% |
|
Disagree |
67 |
17.2% |
|
Not Sure |
105 |
27% |
|
Receiving training in breast exam |
20 |
5.1% |
|
History of doing BSE |
91 |
23.4% |
|
Frequency of doing BSE |
||
|
Once per month |
55 |
60.4% |
|
Once every 2 months |
8 |
8.8% |
|
Once every 6 months |
22 |
24.2% |
|
Once per year |
6 |
6.6% |
|
Total |
91 |
100% |
|
Advising friends to do the BSE |
110 |
28.3% |
|
Overall score of practice towards BSE |
- |
34.60% |
Table 4: Practice towards breast cancer and BSE among Sudanese females attended to OMH.
|
Family History of Bca |
History of doing BSE |
Total |
|
|
YES |
NO |
||
|
Yes |
33 |
67 |
100 |
|
36.3% |
22.5% |
25.7% |
|
|
No |
58 |
231 |
289 |
|
63.7% |
77.5% |
74.3% |
|
|
Total |
91% |
298% |
3895% |
|
100.0% |
100.0% |
100.0% |
|
|
Note: P value=0.008. |
|||
Table 5: Correlation between family history of breast cancer and history of doing BSE.
|
Education |
History of doing BSE |
Total |
|
|
YES |
NO |
||
|
Illiterate |
0% |
7% |
7% |
|
|
0.0% |
100.0% |
100.0% |
|
Basic |
4% |
40% |
44% |
|
|
9.1% |
90.9% |
100.0% |
|
Secondary |
20 |
148 |
168 |
|
|
11.9% |
88.1% |
100.0% |
|
University |
63 |
99 |
162 |
|
|
38.9% |
61.1% |
100.0% |
|
Postgraduates |
4% |
4% |
8% |
|
|
50.0% |
50.0% |
100.0% |
|
Total |
91% |
298% |
389% |
|
23.4% |
76.6% |
100.0% |
|
|
Note: P value=0.000. |
|||
Table 6: Correlation between level of education and history of doing BSE.
|
Personal History of otherBreast Disease |
History of doing BSE |
Total |
|
|
Yes |
No |
||
|
Yes |
10% |
14% |
24% |
|
41.70% |
58.30% |
100.00% |
|
|
No |
81% |
284 |
365 |
|
22.20% |
77.80% |
100.00% |
|
|
Total |
91% |
298% |
389% |
|
23.40% |
76.60% |
100.00% |
|
|
Note: P value=0.029. |
|||
Table 7: Correlation of personal history of other breast disease and history of doing BSE.
|
Did you receive training/ counselling about method of the examination |
History of doing BSE |
Total |
|
|
Yes |
No |
||
|
Yes |
13% |
7% |
20% |
|
65.0% |
35.0% |
100.0% |
|
|
No |
78% |
291% |
369% |
|
21.1% |
78.9% |
100.0% |
|
|
Total |
91% |
298% |
389% |
|
23.4% |
76.6% |
100.0% |
|
|
Note: P value=0.000. |
|||
Table 8: Correlation history of doing BSE and receiving training or counseling about BSE.
|
Training about method of the examination |
You are afraid that you'll detect breast cancer |
Total |
||
|
AGREE |
DISAGREE |
NOT SURE |
||
|
Yes |
12 |
5 |
3 |
20 |
|
60.00% |
25.00% |
15.00% |
100.00% |
|
|
No |
96 |
159 |
114 |
369 |
|
26.00% |
43.10% |
30.90% |
100.00% |
|
|
Total |
108 |
164 |
117 |
389 |
|
27.80% |
42.20% |
30.10% |
100.00% |
|
|
Note: P value=0.004. |
||||
Table 9: Correlation between receiving training counseling about method of BSE and fear of detecting the breast cancer.
|
Education |
You are afraid that you'll detect breast cancer |
Total |
||
|
Agree |
Disagree |
Not Sure |
||
|
Illiterate |
1 |
1 |
5 |
7 |
|
14.30% |
14.30% |
71.40% |
100.00% |
|
|
Basic |
9 |
8 |
27 |
44 |
|
20.50% |
18.20% |
61.40% |
100.00% |
|
|
Secondary |
45 |
64 |
59 |
168 |
|
26.80% |
38.10% |
35.10% |
100.00% |
|
|
University |
51 |
85 |
26 |
162 |
|
31.50% |
52.50% |
16.00% |
100.00% |
|
|
Postgraduates |
2 |
6 |
0 |
8 |
|
25.00% |
75.00% |
0.00% |
100.00% |
|
|
Total |
108 |
164 |
117 |
389 |
|
27.80% |
42.20% |
30.10% |
100.00%
|
|
|
Note: P Value=0.000. |
||||
Table 10: Correlation between education and fear of detecting the breast cancer.
|
Family History of Bca |
You are afraid that you'll detect breast cancer |
Total |
||
|
Agree |
Disagree |
Not Sure |
||
|
YES |
40 |
39 |
21 |
100 |
|
40.0% |
39.0% |
21.0% |
100.0% |
|
|
NO |
68 |
125 |
96 |
289 |
|
23.5% |
43.3% |
33.2% |
100.0% |
|
|
Total |
108 |
164 |
117 |
389 |
|
27.8% |
42.2% |
30.1% |
100.0% |
|
|
Note: P Value=0.004 |
||||
Table 11: Correlation between family history of breast cancer and fear of detecting the breast cancer.
|
History of other Breast Disease |
Fear of detecting the breast cancer |
Total |
||
|
Agree |
Disagree |
Not Sure |
||
|
Yes |
8 |
12 |
4 |
24 |
|
33.30% |
50.00% |
16.70% |
100.00% |
|
|
No |
100 |
152 |
113 |
365 |
|
27.40% |
41.60% |
31.00% |
100.00% |
|
|
Total |
108 |
164 |
117 |
389 |
|
27.80% |
42.20% |
30.10% |
100.00%
|
|
|
Note: P value=0.335 |
||||
Table 12: Correlation between history of breast disease and fear of detecting the breast cancer.
|
Education |
Hearing about breast cancer |
Total |
|
|
YES |
NO |
||
|
Illiterate |
6 |
1 |
7 |
|
85.70% |
14.30% |
100.00% |
|
|
Basic |
39 |
5 |
44 |
|
88.60% |
11.40% |
100.00% |
|
|
Secondary |
162 |
6 |
168 |
|
96.40% |
3.60% |
100.00% |
|
|
University |
161 |
1 |
162 |
|
99.40% |
0.60% |
100.00% |
|
|
Postgraduates |
8 |
0 |
8 |
|
100.00% |
0.00% |
100.00% |
|
|
Total |
376 |
13 |
389 |
|
96.70% |
3.30% |
100.00% |
|
|
Note: P value=0.004 |
|||
Table 13: Correlation between hearing about breast cancer and education.
|
Family History of Bca |
Ever heard of BSE |
Total |
|
|
YES |
NO |
||
|
YES |
79 |
21 |
100 |
|
79.0% |
21.0% |
100.0% |
|
|
NO |
195 |
94 |
289 |
|
67.5% |
32.5% |
100.0% |
|
|
Total |
274 |
115 |
389 |
|
70.4% |
29.6% |
100.0% |
|
|
Note: P value=0.019 |
|||
Table 14: Correlation between hearing about BSE and family history of breast cancer.
|
Do You infect by any Sort of Breast Disease |
Ever heard of BSE |
Total |
|
|
YES |
NO |
||
|
Yes |
20 |
4 |
24 |
|
83.30% |
16.70% |
100.00% |
|
|
No |
254 |
111 |
365 |
|
69.60% |
30.40% |
100.00% |
|
|
Total
|
274 |
115 |
389 |
|
70.40% |
29.60% |
100.00% |
|
|
Note: P value=0.153 |
|||
Table 15: Correlation between hearing about BSE and history of breast disease.
|
Sources of information on BSE |
Education |
Total |
||||
|
Illiterate |
Basic |
Secondary |
University |
Postgraduates |
||
|
Tv/Radio |
0 |
8 |
54 |
49 |
4% |
115% |
|
0.0% |
53.3% |
48.6% |
34.5% |
50.0% |
41.5% |
|
|
Health Cadre |
0% |
0% |
19 |
39 |
1% |
59% |
|
0.0% |
0.0% |
17.1% |
27.5% |
12.5% |
21.3% |
|
|
Family/Friends |
1 |
6 |
27 |
16 |
1% |
51% |
|
100.0% |
40.0% |
24.3% |
11.3% |
12.5% |
18.4% |
|
|
Educational Prints |
0.0% |
0.0% |
0.6% |
23% |
2% |
31% |
|
.0% |
.0% |
5.4% |
16.2% |
25.0% |
11.2% |
|
|
Net |
0.0% |
1% |
5% |
15% |
0% |
21% |
|
0.0% |
6.7% |
4.5% |
10.6% |
0.0% |
7.6% |
|
|
Total |
1% |
15% |
111% |
142% |
8% |
277% |
|
100.0% |
100.0% |
100.0% |
100.0% |
100.0% |
100.0% |
|
|
Note:P value=0.001 |
||||||
Table 16: Correlation between source of information about BSE and education.
|
Sources of information on BSE |
OCCUPATION |
Total |
||||
|
STUDENT |
HOUSE WIFE |
WORKER |
EMPLOYEE |
OTHERS |
||
|
TV/ Radio |
5 |
66 |
19 |
23 |
2 |
115 |
|
33.3% |
44.3% |
44.2% |
37.7% |
22.2% |
41.5% |
|
|
Health Cadre |
3 |
26 |
9 |
16 |
5 |
59 |
|
20.0% |
17.4% |
20.9% |
26.2% |
55.6% |
21.3% |
|
|
Family/Friends |
2 |
35 |
9 |
5 |
0 |
51 |
|
13.3% |
23.5% |
20.9% |
8.2% |
.0% |
18.4% |
|
|
Educational Prints |
3 |
9 |
3 |
14 |
2 |
31 |
|
20.0% |
6.0% |
7.0% |
23.0% |
22.2% |
11.2% |
|
|
Net |
2 |
13 |
3 |
3 |
0 |
21 |
|
13.3% |
8.7% |
7.0% |
4.9% |
0.0% |
7.6% |
|
|
Total |
15 |
149 |
43 |
61 |
9 |
277 |
|
100.0% |
100.0% |
100.0% |
100.0% |
100.0% |
100.0% |
|
|
Note: P value=0.011 |
||||||
Table 17: Correlation between source of information about BSE and occupation.
|
Age Group |
Ever heard of BSE |
Total |
|
|
Yes |
No |
||
|
< 20 |
2 |
7 |
9 |
|
22.2% |
77.8% |
100.0% |
|
|
20-30 |
161 |
63 |
224 |
|
71.9% |
28.1% |
100.0% |
|
|
31-40 |
89 |
36 |
125 |
|
71.2% |
28.8% |
100.0% |
|
|
41-50 |
15 |
8 |
23 |
|
65.2% |
34.8% |
100.0% |
|
|
> 50 |
7 |
1 |
8 |
|
87.5% |
12.5% |
100.0% |
|
|
Total |
274 |
115 |
389 |
|
70.4% |
29.6% |
100.0% |
|
|
Note: P value=0.020 |
|||
Table 18: Correlation age groups and ever hearing about breast self-examination.
|
Age Group |
You are afraid that you'll detect breast cancer |
Total |
||
|
Agree |
Disagree |
Not Sure |
||
|
< 20 |
3 |
4 |
2 |
9 |
|
|
33.3% |
44.4% |
22.2% |
100.0% |
|
20-30 |
65 |
96 |
63 |
224 |
|
|
29.0% |
42.9% |
28.1% |
100.0% |
|
31-40 |
33 |
54 |
38 |
125 |
|
|
26.4% |
43.2% |
30.4% |
100.0% |
|
41-50 |
6 |
7 |
10 |
23 |
|
|
26.1% |
30.4% |
43.5% |
100.0% |
|
> 50 |
1 |
3 |
4 |
8 |
|
|
12.5% |
37.5% |
50.0% |
100.0% |
|
Total |
108 |
164 |
117 |
389 |
|
27.8% |
42.2% |
30.1% |
100.0% |
|
|
Note: P value=0.782. |
||||
Table 19: Correlation age groups and fear of detecting breast cancer.
Citation: Kunna A, Ismail KS, Enour S, Taha U, Elkheir HA, et al. (2019) Knowledge, Attitude and Practice of Breast Self-Examination Among Sudanese Females Attended to Omdurman Maternity Hospital in Sudan. Ann Med & Surg Case Rep: AMSCR-1000020.
