
Annals of Medical & Surgical Case Reports
Esophageal Metastasis of Rectal Cancer: A Case Report and Literature Review
Nisrine Acharfi1*, Raihanna Boujarnija1, Karima Oualla1, Zineb Benbrahim1, Samia Arifi1, Hind El fatemi2, Meryem Boubou3, Zahra Bouhnoun4, Mohammed El Abkari4, Adil Ibrahimi4 and Nawfel Mellas1
1Department of Medical Oncology, Hassan II University Hospital, Fez, Morocco
2Department of Pathology, Hassan II University Hospital, Fez, Morocco
3Department of Radiology, Hassan II University Hospital, Fez, Morocco
4Department of Gastro enterology, Hassan II Hospital, Fez, Morocco
*Corresponding author: Nisrine Acharfi, Department of Medical Oncology, Hassan II University Hospital, Fez, Morocco, Tel: +212652210247.
Citation: Acharfi N (2019) Esophageal Metastasis of Rectal Cancer: A Case Report and Literature Review. Ann Med & Surg Case Rep: AMSCR: 100003
Received Date: 01 April, 2019; Accepted Date: 08 April, 2019; Published Date: 18 April, 2019
Abstract
Esophageal metastases are rare. We report the case of a patient with a secondary oesophageal localization of a rectal adenocarcinoma collated in the medical oncology department of CHU HASSAN II of Fez. The patient had a dysphagia of 1 month. Endoscopy digestive had objectified an esophageal tumor. An histological examination had confirmed the metastatic esophageal nature of a rectal cancer. But considering the presence of multiple metastatic sites in the liver and lung. A palliative chemotherapy was started. She died two weeks later. The aim of this work is to show the rarity of this entity and describe the clinical, radiological, pathological, and prognostic features, in addition to therapeutic management.
Keywords: Dysphagia; Rectal cancer; Esophageal metastases
Introduction
The incidence of esophageal metastases is low [1]. These can be confused with benign oesophageal stenosis or primary cancer of the esophagus hence the interest of digestive fibroscopy with biopsy [2]. Few patients remain candidates for curative resection [3].
Case Presentation
We report a case of 37-year-old women treated in the department of medical oncology at Hassan II University hospital in Fez for adenocarcinoma of rectum who initially received a concomitant radiochemotherapy and operated after having undergone anterior resection of the rectum with colo anal anastomosis.
One year after, the patient had bone liver and lung metastases. She received first line chemotherapy 4 cycles of XELOX.
After three weeks of the last course of treatment, a patient presented with progressively worsening dysphagia associated with postprandial vomiting. The fibroscopy objectified a stenosaloesophageal tumor.
The biopsy and an anathomopathological study objectified an oesophageal location of a moderately differentiated and infiltrating adenocarcinoma.
The evaluation radiological assessment showed the appearance of oesophageal thickening and the progression of secondary pulmonary localizations (Figure)
Tumor markers were high. After the completion of a feeding jejunostomy, second-line chemotherapy with FOLFIRI was initiated. After a single cycle, the patient died. The survival of this patient was 1 month after the discovery of oesophageal metastases.
Discussion
The first case of esophageal metastasis that has been described in the literature is that of a prostatic primitive [4]. Other cases of various primitives have been reported including the breast [5] the ovarian [6] the lung [7] and the liver cancers [8].
Esophageal metastases of colorectal cancer are rare. Some cases have been reported in the literature [1,9-11]. In autopsy series their incidence was 0.3 to 6% [2,12].
The mechanisms of dissemination and appearance of these oesophageal metastases are hematogenous and lymphatic [1].
Clinically, esophageal metastases are revealed by dysphagia, vomiting and hematemesis [13]. Esophageal infiltration is most often located in the submucosal region [2].
Digestive endoscopy shows the presence of luminal stenoses with an overlying normal mucosa, often making the histological diagnosis difficult [13]. The abdominal thoraco scan shows a concentric thickening of the esophageal wall, a narrowing of the esophageal lumen without apparent extrinsic mass [14].
In our patient, the biopsies showed an oesophageal mucosa infiltrated with carcinomatous tumor proliferation arranged in glands and cribiform massifs.
There is no therapeutic standard for the treatment of oesophageal metastases. However, local radiotherapy or systemic chemotherapy may be initiated because of the multiplicity of metastatic sites [3].
Surgery type oesophagectomy may be recommended in case of early tumor slowly evolving. Esophageal stents may also be made and proposed to patients as a palliative strategy [15].
Surgical resection of metastatic lesions of other organs remains difficult due to lack of clinical benefit and high morbidity [1]. In our patient, because of the presence of bone and pulmonary liver metastases, we opted for palliative chemotherapy.
Conclusion
Esophageal metastases of colorectal cancer remain rare. Thus any dysphagia in a patient with colorectal cancer will require a gastrointestinal endoscopy with multiple biopsies.
The treatment of esophageal metastases and their prognosis are mainly based on the nature of the primitive and the distance extension assessment.
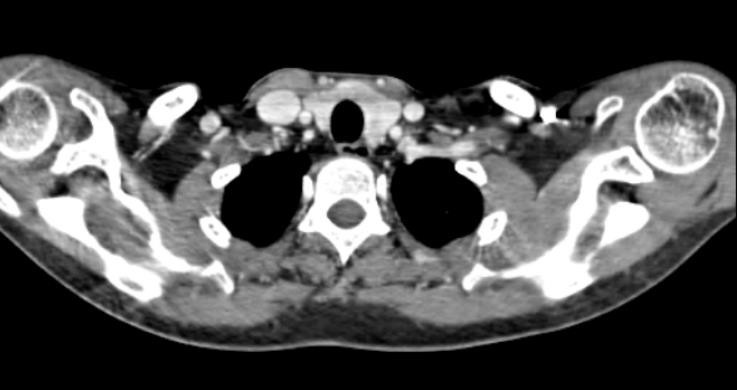
Figure: Abdominal CT showing an oesophageal thickening.
References
Citation: Acharfi N (2019) Esophageal Metastasis of Rectal Cancer: A Case Report and Literature Review. Ann Med & Surg Case Rep: AMSCR: 100003
