
Australian Journal of Nursing Research
(ISSN 2652-9386)
Research Article
Daytime Sleepiness among Adolescents in Six Asian Regions: A Cross-Sectional Survey
Takeuchi S1, Tanida K1, Ikeda M1, Miyagawa S2, Nagai T3, Mekviwattanawong C4, Phuphaibul R4, Nailes JM5, Ligot J6, Chien WT7 and Lee RLT8*
1College of Nursing Art and Science” in Japan
2Doshisha Women’s College of Liberal Arts, Kyotanabe, Kyoto, Japan
3Faculty of Humanistic Education, St. Andrew’s University of Education, Osaka, Japan
4Faculty of Medicine, Mahidol University, World Health Organization Collaborating Center, Bangkok, Thailand
5University of the East Ramon Magsaysay Memorial Medical Center Inc., Quezon City, Philippines
6The University of the Philippines-Manila, College of Public Health, Manila, Philippines
7The Nethersole School of Nursing, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong SAR, China
8School of Nursing and Midwifery, Faculty of Health and Medicine, The University of Newcastle, Callaghan, New South Wales, Australia
*Corresponding author: Regina LT Lee, Professor in Nursing, Faculty of Health and Medicine, School of Nursing and Midwifery, University of Newcastle, Callaghan, New South Wales, 2308 Australia.
Citation: Lee RLT, et al. (2020) Daytime Sleepiness among Adolescents in Six Asian Regions: A Cross-Sectional Survey. Aus J Nursing Res AJNR-100023
Received date: 18 December, 2020; Accepted date: 22 December, 2020; Published date: 29 December, 2020
Abstract
This study aimed to examine the prevalence and compare the correlates of daytime sleepiness among adolescents in six Asia regions in China, Hong Kong, Taiwan, Japan, Philippines and Thailand between 2015 and 2016, using the Pediatric Daytime Sleepiness Scale (PDSS). Data were analyzed for 18,532 children aged 10–15 years. The overall median PDSS score was 15.0, and median scores differed significantly among the six regions. Individual characteristics significantly associated with higher daytime sleepiness were greater age, female, low body mass index, employment status, greater internet usage, living separately from parents, negative feelings regarding relationships with others, and lower parental education. In the binomial logistic regression, 10-year-old children were significantly less likely to have excessive daytime sleepiness than 12 to 15-year-old children. The findings suggest that daytime sleepiness in Asian adolescents differed by region and individual characteristics and increased with age in normal life. This study draws attention to an urgent need for policies related to daytime sleepiness in Asian adolescents that focus on regional profiles and individual characteristics.
Keywords: Adolescents; Asian; Excess daytime sleepiness; Sleep
Introduction
Excessive daytime sleepiness affects 40% of children and adolescents globally [1,2]. Daytime sleepiness is a condition caused by a desire for sleep at inappropriate times, which is followed by cognitive and behavioral problems because of impaired sleep quality or inadequate sleep and sleep hygiene [3]. Daytime sleepiness causes impact on the adolescents’ health-related functions, such as poor academic performance, increased school absenteeism and reported frequent body discomforts [4]. The risk factors of excessive daytime sleepiness in adolescents are short sleep duration and health perception with chronic insufficient sleep for a period of time [5]. Moreover, previous studies have demonstrated several mechanisms underlying adolescent daytime sleepiness, including continuous daily delay in bedtime owing to social activities and exposure to light at night, modulation of the 24-hour biological clock, and advanced technological devices that impair adolescents’ bedtime (Adolescent Sleep Working Group, 2014). It has also found that excessive day time sleepiness caused by changes in hormonal balance during the development of secondary sexual characteristics in puberty [6]. Thus, puberty plays a critical role in the development of excessive daytime sleep and it causes a major health concern during adolescence.
Literature review
Little is known about sleep patterns and problems in Asian adolescents. The etiology of daytime sleepiness is likely to be complex and interrelated with many physical and social environmental risk factors. Thus, there is an urgent need to examine the prevalence and risk factors contributing to excessive daytime sleepiness during adolescence as it increases with age among Asian adolescents. Previous studies reported that the detailed interactions and correlations of risk factors associated with excessive daytime sleepiness were insufficient sleep [7,8], sleep disturbances [9], lifestyle factors [10] and physical environment [11]. Nonetheless, the detailed interactions of puberty with these multiple factors, especially on the occurrence of daytime sleepiness during adolescence remain unclear.
It has been found that Asian adolescents’ bedtimes are later than their peers from North America and Europe, resulting in less total sleep time on school nights and a tendency for higher rates of daytime sleepiness [12]. Moreover, an investigation of the causes of daytime sleepiness and strategies to overcome this problem during adolescence would not only have academic benefits, but also socio-economic benefits, such as maintaining and improving the health of adolescent children, reducing medical costs, and generating social benefits through diversity and improvement of their activities [13].
Furthermore, an international cross-sectional survey may allow researchers to compare several different variables in relation to physical, psychosocial, and social activities because adolescent daytime sleepiness is affected by these three factors. However, there were no cross-country surveys comparing the Asian adolescents’ sleep hygiene including the prevalence and correlates have been performed to date. Hence, the researchers from six regions collaborated and conducted an international cross-sectional survey to study daytime sleepiness among adolescents in six Asia regions.
Study aim: This study aimed to examine the prevalence and compare the correlates of daytime sleepiness among adolescents in six Asia regions in China, Hong Kong, Taiwan, Japan, Philippines and Thailand. Three of them were the World Health Organization (WHO) Collaborating Centers from the Western Pacific and South East Asia Regions including Hong Kong, Japan and Thailand. The other three institutes were academic research institutes in the WHO’s educational institution networks. The researchers from these six Asia regions formed a research group and aimed to promote the health and wellbeing of children and adolescents in the regions in order to help to achieve the United Nation’s Sustainable Development Goal 3 through promoting sleep hygiene to promote wellbeing and ensure healthy lives (United Nation, 2018). A cross-sectional survey focused on health-related lifestyles and psychosocial health behaviors among Asian adolescents in these six regions conducted in 2017. The focus of this paper is to report the findings of data analysis related to daytime sleepiness among the adolescents from these six Asia regions.
Materials and Methods
Design: The present study had an international cross-sectional survey design, including a battery of anonymous self-reported questionnaires.
Study participants: Participants were recruited from elementary schools and junior high schools in six Asian regions including Zhengzhou in China; Hong Kong; Taipei in Taiwan; Kansai region in Japan; Manila in Philippines; and Bangkok in Thailand. The inclusion criteria of the study samples were students in grades 4 to 9 in primary and secondary schools. Children were excluded if they were 9 years old or younger because the World Health Organization defines adolescents as people aged 10-19 years (World Health Organization, 1998). This survey was conducted by six Asia regions in China, Hong Kong, Taiwan, Japan, Philippines, and Thailand between 2015 and 2016. After ethical approvals were obtained from each of the participating institutions, each site recruited at least 1,500 participants aged 8-15 years, with a total sample size of 21,359. Participants were conveniently recruited in each region. Each region recruited their sample based on the study inclusion and exclusion criteria.
Data collection: Either the schoolteachers in the participated schools or the research team distributed the questionnaires to the participants. Participants were allowed to complete the questionnaires at their school, children’s center or home. Their school teachers, parents and the research team when necessary provided the participants support. The schoolteachers, principals or children’s center staff collected the completed questionnaires from the participants and returned them to the research team.
Measures: The study instruments included a demographic sheet to describe the characteristics of study sample and the Pediatric Daytime Sleepiness Scale [14]. The English-language version of the questionnaires was translated into the participants’ mother language and then translated back into English to check for accuracy by the research team of each region.
Demographic Sheet: The demographic sheet included the participant’s age, gender, study class, time spent on the internet (h/day), and mothers’ and fathers’ education level. Body mass index (BMI) was calculated from weight (kg) divided by height (m) squared, and was classified into three categories as defined by the World Health Organization (WHO, 2007): thin and severely thin; normal; and overweight and obese. Participants were classified as living with parent(s) if they were living with their parent(s), including step-parent(s), and other persons (siblings, grandparents and other relatives), and as not living with parent(s) if they were living with grandparents and/or other relatives, or if they were living in a dormitory. For the question about feelings regarding the relationship with their mothers, fathers and schoolteachers, multiple answers were allowed. The questions contained four positive sided items (affectionate, trusting, clearly communicated values, and able to deal with conflicts) and six negative sided items (difference in values, non-communicative, distant relationship, poor relationship, constant struggle, and definite conflicts). The researchers classified those items to three categories: 1) one-sided; positive, 2) both positive and negative and 3) one-sided; negative. Participants were classified as one-sided; positive if they selected some items from positive sided items, as both positive and negative if they selected some items from both positive and negative sided items, and as one-sided; negative if they selected some items from negative sided items. The following variables were not measured in the following some cities due to ethical issues or technical problems. BMI measurement was excluded in Thailand; living situation and feelings regarding the relationship with their mothers, fathers and schoolteachers were excluded in the Philippines; and mothers’ education level and fathers’ education level were excluded in Japan.
Pediatric Daytime Sleepiness Scale: The PDSS aims to develop a measure of daytime sleepiness suitable for middle-school children and examine the relationship between daytime sleepiness and school-related outcomes (Drakes et al., 2003). The PDSS includes eight items related to sleepiness behaviors and was developed as a self-report measure in samples aged 10-15 years old. The eight items of the PDSS are as follows: 1) How often do you fall asleep or get drowsy during class periods? 2) How often do you get sleepy or drowsy while doing your homework? 3) Are you usually alert most of the day? 4) How often are you ever tired and grumpy during the day? 5) How often do you have trouble getting out of bed in the morning? 6) How often do you fall back to sleep after being awakened in the morning? 7) How often do you need someone to awaken you in the morning? and 8) How often do you think that you need more sleep? All questions were presented in a 5-point Likert Scale format (never=0, seldom=1, sometimes=2, frequently=3, always=4). Scores ranged from 0 to 32 and it is based on the manual for the PDSS [14]. In this study, the researchers classified PDSS scores as low or high using 21 as the cutoff in the binomial logistic regression. Higher scores indicate greater sleepiness [14]. Internal consistency reported with Cronbach’s alpha was 0.80 for the PDSS in the full sample in this study. The international consistency of the PDSS for the original publication was 0.80 [15].
Data analysis: The distribution of PDSS scores in the six Asian regions was confirmed using the Kolmogorov-Smirnov test. To assess differences between regions, we compared total PDSS scores using the Kruskal-Wallis test. Moreover, to assess differences according to participant characteristics, we compared total PDSS scores using the Kruskal-Wallis and Mann-Whitney U tests for categorical variables and simple linear regression analysis for continuous variables. Furthermore, we used binomial logistic regression to assess the association between characteristics and pediatric daytime sleepiness. Each independent variable was applied via simultaneous forced entry. A p-value of less than 0.05 indicated significance. Statistical analyses were performed using IBM SPSS Statistics version 22.0.
Ethical considerations: The protocol for the research project has been approved suitably constituted research ethics committee of the institutions within which the work was undertaken. Ethical approvals were obtained from the following ethics committees prior to data collection. These Committees include The Hong Kong Polytechnic University, Faculty Research Committee, Hong Kong with the Approval No: HSEARS20150619002 in Hong Kong; the Research Ethics Committee of the College of Nursing Art and Science, the Research Institute of Nursing Care for People and Community in Japan with the Approval No: 2015 F12 3; the UERM Research Institute for Health Sciences in Philippines with the Ethics Review Committee Approval No: 0318/E/M/16/60; the Ethics Committee of the Faculty of Medicine Ramathibodi Hospital, Mahidol University, Thailand. Besides the study information sheet, the research team in each region also provided a verbal briefing session and explained the study aim and the purpose of each study tool to the principals of elementary schools, junior high schools and children’s centers. After seeking permission from the school principals, the research team in each region provided a briefing to schoolteachers using the same study information sheet. Written informed consent was obtained from all parents through each school’s communication system. The participants could withdraw from the study without penalty during the data collection.
Results
In total, 20,479 children aged 9-15 years returned the questionnaire. In this study, we excluded 750 children aged 9 years or younger, 136 children who lacked age information and 1,061 children with incomplete PDSS responses. Thus, data were analyzed for 18,532 children aged 10-15 years. The characteristics of the study participants showed in (Table 1).
Adolescent daytime sleepiness: The patterns of the PDSS scores in the six Asian regions is shown in Table 2. Significant differences were observed for adolescent daytime sleepiness among the six Asian regions (p<0.001). In ascending order, the median PDSS scores were 12.0 (interquartile range [IQR] 6.0-17.0) for China, 14.0 (IQR 8.0-18.0) for Taiwan, 16.0 (IQR 11.0-19.0) for Hong Kong, 16.0 (IQR 2.0-20.0) for Japan, 17.0 (IQR 13.0-21.0) for Thailand, and 17.0 (IQR 14.0-21.0) for the Philippines.
Comparison of adolescent daytime sleepiness by participant characteristics: In this study, the PDSS score correlated with age, gender, BMI, employment status, living situation, feelings regarding the relationship with their mothers, fathers and schoolteachers, mothers’ and fathers’ education level and time spent on the internet (Figure 1 and Figure 2). From 10 to 15 years of age, PDSS score was increased significantly with increased age (Figure 1A).
PDSS scores in females were significantly higher than in males (Figure 1B). PDSS scores in overweight and obese participants were significantly lower than those in normal, thin and severely thin participants (Figure 1C). PDSS scores in participants who were employed was significantly higher than that in those who were not employed (Figure 1D). PDSS scores in those living separately from their parent(s) were higher than in those living with their parent(s) (Figure 1E). PDSS scores in one-sided; negative items scored significantly higher than one-sided; positive and both positive and negative items (Figure 1F, 1G and 1H). PDSS scores in mothers’ education level of completed primary school or equivalent was significantly higher than that in mothers’ education level of completed secondary/junior high school and completed secondary/high school (Figure 1I). PDSS scores in fathers’ education level of completed primary school or equivalent was significantly higher than that in fathers’ education level of completed secondary/junior high school, completed secondary/high school and completed tertiary school (Figure 1J). Time spent on the internet was positively associated with PDSS score (Figure 2).
Associations between adolescent daytime sleepiness and participant characteristics: Among the 18,532 adolescents analyzed in this study, the data from those in China, Taiwan and Hong Kong with missing data were excluded from the logistic regression. The data of adolescents in Japan, the Philippines and Thailand were excluded from the binomial logistic regression because some variables were not measured in the questionnaire. Our final sample for the binomial logistic regression comprised 7,736 children in China, Taiwan and Hong Kong. The model chi-square test showed p<0.05?the Hosmer and Lemes how test showed p=0.087, and the predictive accuracy was 85.8% as shown in Table 3.
The results of this study found that age, gender, BMI, time spent on the internet, employment status, living situation, mothers’ education level, fathers’ education level, feelings regarding the relationships with their mothers, fathers and schoolteachers, and country were significantly associated with the PDSS (Table 3).
In this study the 10-year-old adolescents were significantly less likely to have excessive daytime sleepiness than those who were 12-year-old adolescents (adjusted odds ratio [OR] 2.45, 95% confidence interval [CI] 1.79-3.35; p<0.001), 13-year-old adolescents (adjusted OR 3.38, 95% CI 2.50-4.56, p<0.001), 14-year-old adolescents (adjusted OR 3.68, 95% CI 2.72-4.99, p<0.001), and 15-year-old adolescents (adjusted OR 4.21, 95% CI 3.07-5.78, p<0.001) as shown in Table 3.
Discussion
This is the first study to describe excessive daytime sleepiness among adolescents aged 10-15 years using data from an international cross-sectional survey in six Asian regions: China, Hong Kong, Taiwan, Japan, the Philippines and Thailand. No cross-country surveys targeting Asian adolescent children have been performed to date in regards to daytime sleepiness. This study shows the status quo of daytime sleepiness in adolescent children in Asia.
For those adolescents between the ages of 10 and 15 years, there were differences among ethnic groups with regard to daytime sleepiness. Although previous studies targeting adult have shown differences among ethnic groups regarding the mechanisms underlying sleep [16] no studies targeting adolescents have been conducted. Our analysis showed a difference between ethnic groups even during adolescence between the ages of 10 and 15 years.
Characteristics of adolescent daytime sleepiness in six Asian regions: Daytime sleepiness was significantly affected by age, gender, BMI, employment status, time spent on the internet each day, and living situation, or the relationships with parents and schoolteachers. Because there are various factors related to daytime sleepiness in adolescent children, it is important to study the effects of each of those factors on individual children.
Adolescents with the ages between 10 to 15 years old, their daytime sleepiness was shown to increase significantly with age. During adolescence, the circadian rhythm shifts from daytime to nighttime; nighttime melatonin secretion is delayed as a result of a constant delay in bedtime owing to multiple reasons, such as increased social activities inside and outside school, homework assignments, and preparation for examinations, thereby causing sleepiness during the daytime (Adolescent Sleep Working Group, 2014); this condition is considered to progress from the age of 10 to 15 years.
Females were found to have significantly higher daytime sleepiness than males. Previous studies have shown that an increase in progesterone secretion after menarche causes a decrease in the quality of sleep at night and induces sleepiness during daytime [17]. The mean age of menarche in the countries investigated in the present study has been reported to be within the range of 12.3 to 13.5 years [18]. The present study included children aged 10-15 years, which is the time period when females enter the menarche stage; this is presumably why the female participants in this study showed a higher level of daytime sleepiness than the males.
Although daytime sleepiness is likely to be associated with obesity [19], daytime sleepiness was the lowest in participants who were overweight and obese, followed by normal, thin and severely thin. Previous studies have shown that daytime sleepiness is significantly associated with short sleep duration [20], which reduces leptin but increases ghrelin and orexin, thereby leading to increased appetite and obesity [21,22]. Moreover, in studies on biological clocks, it has been indicated that light, meals, and social activities are synchronous factors [23]. Furthermore, the lack of synchronous factors affects the biological clock, resulting in sleepiness during daytime [24]. Thus, although obesity and daytime sleepiness can occur due to short sleep duration, daytime sleepiness may be lower in obese children as a result of surpassing the synchronization effect of eating behavior on the biological clock. Therefore, it is important to examine the interrelationships among sleepiness, sleep duration, mealtime and BMI.
When the duration of light received due to internet usage was an hour, daytime sleepiness was higher than that due to internet usage for
This study found that daytime sleepiness was lower in participants with positive feelings regarding their relationships with others. Previous studies have shown that a more stable emotional state is correlated with better quality of sleep and lower daytime sleepiness [26]. This is presumably because more a stable emotional state is correlated with positive feelings regarding relationships with others. Therefore, it is important to examine the connection between emotional state and relationships with others.
This study also found that when parents’ education levels were restricted to elementary school level, the child’s daytime sleepiness was significantly higher than those whose parents had received higher education. These results were similar to those of a study that showed a correlation between parental education level and child health [27].
Associations between adolescent excessive daytime sleepiness and participants characteristics: This study found that higher age was significantly associated with excessive daytime sleepiness. To our knowledge, there are no data suggesting that there are genetic factors associated with the development of the brain and other organs that could increase daytime sleepiness. If these were so, the observed age-dependent increase in daytime sleepiness would appear to be attributable to acquired activity patterns, such as shortened sleep time or increased nighttime activity due to increases in social activity with age. Therefore, it is important to examine the relationship between increased age and acquired activity patterns.
Limitations
Our study had several potential limitations. First, our aim was to clarify the status quo of daytime sleepiness in adolescent children in Asia. This survey would ideally have had stratified random sampling or cluster sampling. There were differences in age and gender among the participants of the six Asian regions in this study; therefore, these factors need to be considered when interpreting the results. Second, some variables were not measured in certain cities due to ethical issues or technical problems. When translating the questionnaire from English to the mother language in some of the countries, two variables were missed and allowing multiple answers for some of the questions in some languages was confusing, leading to inaccurate responses. A more detailed study procedure including confirmation of the meanings and the number of questions in the final questionnaire in different languages and for each country should be developed to avoid technical problems in future studies.
Conclusion
Daytime sleepiness in adolescent children from six Asian regions showed a varying trend across regions, which was affected significantly by age, gender, BMI, time spent on the internet, employment status, living situation, mothers’ and fathers’ education level, and their relationships with their parents and schoolteachers. Because greater age was significantly associated with excessive daytime sleepiness, Asian adolescents can become sleepy with increased age in normal life. The WHO has been providing guidance to support countries in improving the health and wellbeing of adolescents to achieve the United Nation’s Sustainable Development Goal No. 3 (United Nation, 2017). This guidance is called the Global Accelerated Action for the Health of Adolescents (AA-HA!) (WHO, 2017). Section 1 of the guidance stresses understanding what is special about adolescents and why investing in them results in long-term societal benefits. Our findings suggest the status quo of daytime sleepiness in adolescent children in Asia differed by region and individual characteristics. Policies related to daytime sleepiness in Asian adolescents with a focus on regional profiles and individual characteristics are urgently needed because daytime sleepiness is associated with a wide range of physical, psychosocial, and social activities among adolescents.
Relevance to Practice
The findings of this study have great public health implications in promoting sleep hygiene for adolescents in Asian countries with the up-to-date evidences. The findings suggest that daytime sleepiness in Asian adolescents differed by region and individual characteristics and increased with age in normal life. This study draws attention to an urgent need for policies related to daytime sleepiness in Asian adolescents that focus on regional profiles and individual characteristics. It is important the role of school nurses adopt these new evidences when planning for future health education and health promotion activities on sleep hygiene in the public health agenda locally and internationally.
Funding Statement
This research was conducted with the support of 1) A grant for child support projects 2015 from KEIAI MACHIZUKURI ZAIDAN in Japan; 2) Central Research Fund, School of Nursing, The Hong Kong Polytechnic University in Hong Kong and 3) Faculty of Medicine, Ramathibodi Hospital, Mahidol University in Thailand.
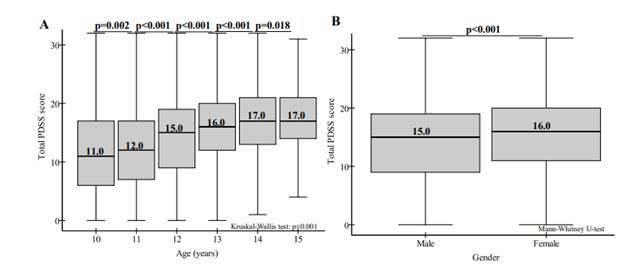
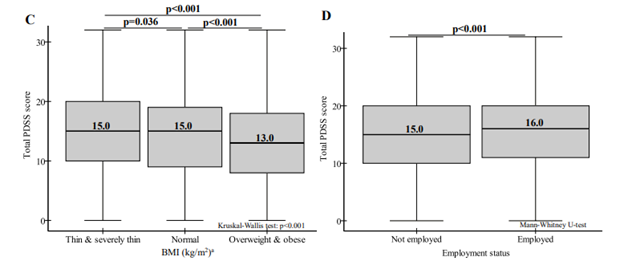
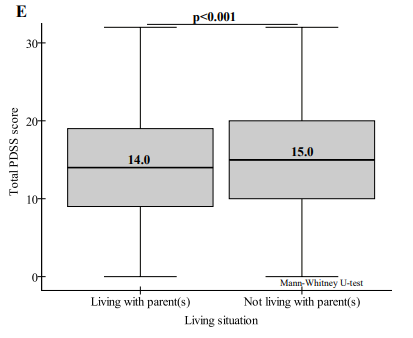
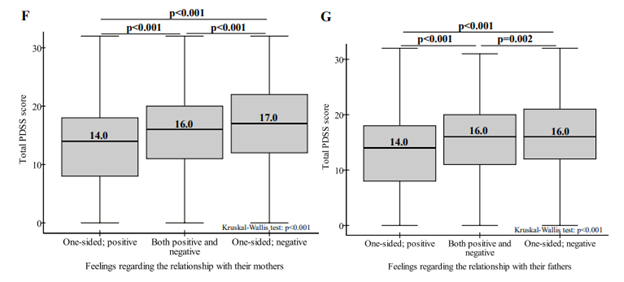
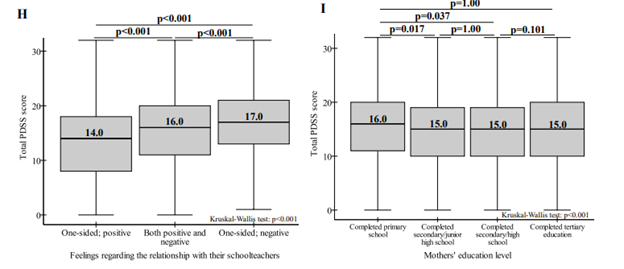
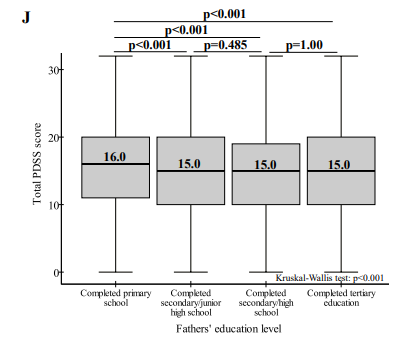
Figure 1: Comparison of adolescent daytime sleepiness by participant characteristics in six Asian regions. The figure reports boxplots, summarizing median (values in each box are medians), interquartile range, minimum and maximum. In part A, p values between continuous ages are shown. In parts B-J, p values among all participants are shown. BMI was classified into three categories as defined by the WHO (2007): thin and severely thin, normal, and overweight and obese.
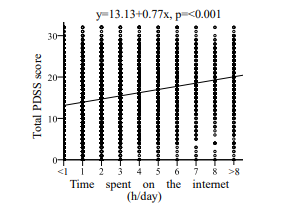
Figure 2: Linear trend effect of time spent on the internet. P values were calculated using simple linear regression. Independent variables were time spent on the internet per day and the dependent variable was PDSS score.
|
Variable |
(N=18,532) |
||
|
n |
(%) |
||
|
Age (years) |
10 |
2,280 |
(12.3) |
|
11 |
2,962 |
(16.0) |
|
|
12 |
3,463 |
(18.7) |
|
|
13 |
3,491 |
(18.8) |
|
|
14 |
3,410 |
(18.4) |
|
|
15 |
2,926 |
(15.8) |
|
|
Gender |
Male |
8,878 |
(48.1) |
|
Female |
9,565 |
(51.9) |
|
|
BMI (kg/m2)a |
Thin & severely thin |
1,064 |
(8.5) |
|
Normal |
8,667 |
(68.9) |
|
|
Overweight & obese |
2,840 |
(22.6) |
|
|
Employment status |
Employed |
748 |
(4.1) |
|
Not employed |
17,485 |
(95.9) |
|
|
Time spent on the internet (h/day) |
<1 |
5,825 |
(33.5) |
|
1 |
3,163 |
(18.3) |
|
|
2 |
2,638 |
(15.2) |
|
|
3 |
1,900 |
(10.9) |
|
|
4 |
1,293 |
(7.4) |
|
|
5 |
991 |
(5.7) |
|
|
6 |
649 |
(3.7) |
|
|
7 |
250 |
(1.4) |
|
|
8 |
213 |
(1.2) |
|
|
>8 |
461 |
(2.7) |
|
|
Living situation |
Living with parent(s) |
13,793 |
(95.1) |
|
Not living with parent(s) |
717 |
(4.9) |
|
|
Feelings regarding the relationship with their mothers |
One-sided; positive |
11,117 |
(80.7) |
|
Both positive and negative |
1,425 |
(10.4) |
|
|
One-sided; negative |
1,228 |
(8.9) |
|
|
Feelings regarding the relationship with their fathers |
One-sided; positive |
10,431 |
(77.7) |
|
Both positive and negative |
1,095 |
(8.2) |
|
|
One-sided; negative |
1,889 |
(14.1) |
|
|
Feelings regarding the relationship with their schoolteachers |
One-sided; positive |
10,802 |
(78.3) |
|
Both positive and negative |
894 |
(6.5) |
|
|
Mothers' education level |
One-sided; negative |
2,093 |
(15.2) |
|
Completed primary school |
1,798 |
(11.0) |
|
|
Completed secondary/junior high school |
3,846 |
(23.7) |
|
|
Completed secondary/high school |
5,533 |
(34.0) |
|
|
Completed tertiary education |
5,085 |
(31.3) |
|
|
Fathers' education level |
Completed primary school |
1,520 |
(9.4) |
|
Completed secondary/junior high school |
3,958 |
(24.4) |
|
|
Completed secondary/high school |
5,379 |
(33.2) |
|
|
Completed tertiary education |
5,343 |
(33.0) |
|
|
Note: BMI=body mass index: BMI was classified into three categories as defined by the WHO (2007): thin and severely thin, normal, and overweight and obese. BMI was excluded in Thailand. Living situation and feelings regarding the relationship with their mothers, their fathers and their schoolteachers were excluded in the Philippines. Mothers' education level and fathers' education level were excluded in Japan. |
|||
Table 1: Participant characteristics.
|
Region |
Total |
China |
Hong Kong |
Taiwan |
Japan |
The Philippines |
Thailand |
|
n |
18,532 |
5,668 |
2,942 |
1,339 |
1,632 |
4,022 |
2,929 |
|
Mean |
14.88 |
11.86 |
15.19 |
13.59 |
15.93 |
17.57 |
16.72 |
|
Median |
15.00 |
12.00 |
16.00 |
14.00 |
16.00 |
17.00 |
17.00 |
|
SD |
6.79 |
7.06 |
6.54 |
6.86 |
6.48 |
5.34 |
5.99 |
|
Note: PDSS: Pediatric Daytime Sleepiness Scale; SD=standard deviation. Total PDSS scores were not normally distributed in all regions. The P value among there six regions was <0.001, calculated by using Kruskal-Wallis test. |
|||||||
Table 2: Summary of PDSS results in six Asian regions.
|
|
|
|
|
n=7,736 |
||
|
Adjusted OR(95%CI)b |
||||||
|
VARIABLE |
p value |
|||||
|
Countrya |
China |
reference |
|
|||
|
Taiwan |
0.37 |
(0.28- |
0.49) |
<0.001 |
||
|
Hong Kong |
0.90 |
(0.76- |
1.06) |
0.204 |
||
|
Age (years) |
10 |
reference |
||||
|
11 |
1.12 |
(0.79- |
1.57) |
0.528 |
||
|
12 |
2.45 |
(1.79- |
3.35) |
<0.001 |
||
|
13 |
3.38 |
(2.50- |
4.56) |
<0.001 |
||
|
14 |
3.68 |
(2.72- |
4.99) |
<0.001 |
||
|
15 |
4.21 |
(3.07- |
5.78) |
<0.001 |
||
|
Gender |
Male |
reference |
||||
|
Female |
1.29 |
(1.13- |
1.48) |
<0.001 |
||
|
BMI (kg/m2)c |
Normal |
reference |
||||
|
Thin & severely thin |
1.03 |
(0.79- |
1.33) |
0.851 |
||
|
Overweight & obese |
1.14 |
(0.96- |
1.35) |
0.130 |
||
|
Time spent on the internet (h/day) |
1.16 |
(1.12- |
1.20) |
<0.001 |
||
|
Employment status |
Not employed |
reference |
||||
|
Employed |
1.28 |
(0.86- |
1.90) |
0.224 |
||
|
Living situation |
Living with parent(s) |
reference |
||||
|
Not living with parent(s) |
1.29 |
(0.92- |
1.80) |
0.134 |
||
|
Feelings regarding the relationship with their mothers |
One-sided; positive |
reference |
||||
|
Both positive and negative |
1.07 |
(0.85- |
1.35) |
0.540 |
||
|
One-sided; negative |
1.51 |
(1.18- |
1.92) |
0.001 |
||
|
Feelings regarding the relationship with their fathers |
One-sided; positive |
reference |
||||
|
Both positive and negative |
1.30 |
(1.01- |
1.67) |
0.038 |
||
|
One-sided; negative |
1.40 |
(1.14- |
1.73) |
0.002 |
||
|
Feelings regarding the relationship with their schoolteachers |
One-sided; positive |
reference |
||||
|
Both positive and negative |
1.43 |
(1.11- |
1.83) |
0.006 |
||
|
One-sided; negative |
1.76 |
(1.45- |
2.13) |
<0.001 |
||
|
Mothers' education level |
Completed primary school |
reference |
||||
|
Completed secondary/junior high school |
1.21 |
(0.93- |
1.57) |
0.154 |
||
|
Completed secondary/high school |
1.34 |
(1.02- |
1.76) |
0.033 |
||
|
Completed tertiary education |
1.24 |
(0.91- |
1.68) |
0.167 |
||
|
Fathers' education level |
Completed primary school |
reference |
||||
|
Completed secondary/junior high school |
1.15 |
(0.85- |
1.57) |
0.367 |
||
|
Completed secondary/high school |
1.00 |
(0.73- |
1.38) |
0.982 |
||
|
Completed tertiary education |
1.22 |
(0.86- |
1.71) |
0.261 |
||
|
Constant |
0.03 |
|
|
<0.001 |
||
|
OR=odds ratio; CI=confidence internal; BMI=body mass index. |
||||||
Citation: Lee RLT, et al. (2020) Daytime Sleepiness among Adolescents in Six Asian Regions: A Cross-Sectional Survey. Aus J Nursing Res AJNR-100023
