
Annals of Medical & Surgical Case Reports
(ISSN: 2652-4414)
Image Article
Pancreato-Gastric Fistula with Bleeding Following Acute Pancreatitis
Ai-Chao Shi1,2, Rong Du1,2, Wei Liu*1,2
1Institute of Digestive Disease, China Three Gorges University, Yichang, China
2Department of Gastroenterology, Yichang Central People’s Hospital, Yichang, China
*Corresponding Author: Wei Liu, Institute of Digestive Disease, China Three Gorges University, 8 Daxue Road, Yichang 443000, China
Citation: Shi AC, Du R, Liu W (2020) Pancreato-Gastric Fistula with Bleeding Following Acute Pancreatitis. Ann Med & Surg Case Rep: AMSCR-100089
Received date: 12 December 2020; Accepted date: 23 December 2020; Published date: 29 December 2020
A 43-year-old man presented to the emergency department with a 1-day history of melena. Three months before presentation, he had presented to the local community hospital with abdominal pain and received a diagnose of severe acute pancreatitis. Physical examination revealed normal vital signs and mild epigastric tenderness with normal bowel sounds.His temperature was 36.6°C, the pulse 69 beats per minute, and his blood pressure 116/75 mm Hg.Laboratory studies showed a hemoglobin level of 10.4 g per deciliter (normal range, 11.5 to 15.5). Computed tomography of the abdomen confirmed pancreatic pseudocyst (Figure A). Considering the ill- defined melena in this patient, gastroscopy was initially assessed and confirmed pancreato-gastric fistula with gastrorrhagia, as well as none bleeding gastric varices which were consistent with left-sided portal hypertension (Figure B, C). A diagnosis of pancreato-gastric fistulawas made. Pancreatic pseudocyst formation is seen in the minority of patients with acute pancreatitis. Walled-off pancreatic necrosis may follow the development of a pseudocyst. Fistulization and spontaneous perforation occur in very few of pseudocysts. Of the rare cases of fistula formation, pacreato-gastric fistulas are the rarest [1]. Understanding the clinical features of pacreato-gastric fistulas and how to manage them is necessary for gastroenterologists. After a well-informed discussion of options for interventions with the patient, the decision was madeto pursue a 2-month course of proton pump inhibitor and gastric mucosa protective agent treatment. After the procedure, he had repeated endoscopy revealing the pancreato-gastric fistula healed and scars left but with persistent gastric varices.
Acknowledgements
Funding: This work was supported by National Natural Science Foundation of China (31600134).
Conflicts of Interest: The authors have no conflicts of interest to declare.
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Written informed consent was obtained from the patient for publication of this “Images in Clinical Medicine”.
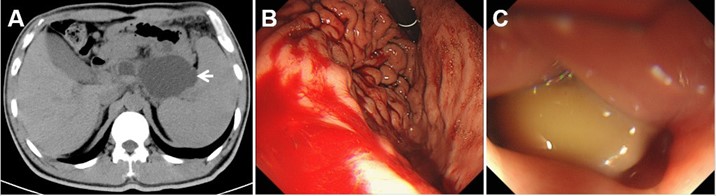
Figure 1: Pancreato-gastric fistula with bleeding following acute pancreatitis. (A) Axial CT image of pancreatic pseudocyst (arrow); (B) gastroscopy revealed pancreato-gastric fistula with gastrorrhagia, as well as gastric varices; (C) pancreato-gastric fistula containing chyme detected by gastroscopy
Citation: Shi AC, Du R, Liu W (2020) Pancreato-Gastric Fistula with Bleeding Following Acute Pancreatitis. Ann Med & Surg Case Rep: AMSCR-100089
