
Journal of Obstetrics and Gynecological Problems
ISSN 2652-466X
Cesarean Scar Sinus Diagnosed as Scar Endometriosis. A Case Report
Fatima N1, Hashmi KS2*, Batool S3, Shabbir N4 and Fatima B5
1Department of Gynaecology and Obstetrics Bahawal Victoria Hospital Bahawalpur Pakistan
2Department of Gynaecology and Obstetrics Bahawal Victoria Hospital Bahawalpur Pakistan
3Department of Gynaecology and Obstetrics Bahawal Victoria Hospital Bahawalpur Pakistan
4Department of Gynaecology and Obstetrics Bahawal Victoria Hospital Bahawalpur Pakistan
5Department of Biochemistry Bahauddin Zakariya University Multan Pakistan
*Corresponding Author: Khiaynat Sarwar Hashmi. Department of Gynaecology and Obstetrics, Bahawal Victoria Hospital, Bahawalpur Pakistan, Tel: +923401966677; Email: ksarwar61@gmail.com
Citation: Fatima N, Hashmi KS, Batool S, Shabbir N, Fatima B (2021) Cesarean Scar Sinus Diagnosed as Scar Endometriosis. A Case Report. J Obstet Gynecol Probl: JOGP 100019
Received date: 05 January, 2021; Accepted date: 29 January, 2021; Published date: 05 February, 2021
Abstract
Endometriosis is a condition that can be explained as an ectopic endometrial tissue. It is well defined as functional endometrial tissue at a site other than endometrial cavity. It usually affects women of reproductive age group as the condition is sex hormone dependant. It is very disturbing condition and prevalent in almost 1-40 % of women in different origins. The common sites of endometriosis were found to be within pelvis especially ovaries, and ligaments of pelvic organs. Scar endometriosis is a rare condition that is often misdiagnosed as other conditions of scar. A 34 year old lady P3 with previous 2 cesarean sections presented in gynae outdoor of Bahawal Victoria Hospital Bahawalpur with chief complaint of painful nodule on the right side of the stitch line.On clinical basis she was diagnosed as scar endometrioma. Her surgery was performed for excision of the nodule and underlying mass. A 3 * 3 cm nodule was excised from subcutaneous tissue. The nodule was sent for histopathology that confirmed the diagnosis.
Keywords: Gastrointestinal tissue; Gynecological/Obstetrical surgeries; Reproductive age; Sex hormone
Introduction
Endometriosis is a condition that can be explained as an ectopic endometrial tissue. It is well defined as functional endometrial tissue at a site other than endometrial cavity [1]. It usually affects women of reproductive age group as the condition is sex hormone dependant. It is very disturbing condition and prevalent in almost 1-40 % of women in different origins [2]. The condition was first described by Rokitansky in 1860. The common sites of endometriosis were found to be within pelvis especially ovaries, and ligaments of pelvic organs. Extra pelvic endometriosis was rare but the prevalent sites were gastrointestinal tissue, lungs, nasal mucosa and abdominal wall more so in scars following obstetrical/ gynecological surgeries [3]. Incidence of abdominal wall endometriosis is very less. Less than 1% [4] .Scar endometriosis is a rare condition that is often misdiagnosed as other conditions of scar.
Case Report
A 34 year old lady P3 with previous 2 cesarean sections presented in gynae outdoor of Bahawal Victoria Hospital Bahawalpur with chief complaint of painful nodule on the right side of the stitch line (Figure 1). Also there was a history of color change and bleeding from that nodule in days of menstruation. She had history of dysmenorrheal and dysparunea present. She had her last cesarean done 18 months back and the history of nodule and bleeding was since then. She had been going to local doctors for the complaint and was prescribed antibiotics and local creams for the wound multiple times. On per abdominal examination there was a pfannensteil incision of about 12 cm and there was a reddish nodule of 1cm on right side of the incision. It was tender and there was discharge present. Under the nodule there was a mass palpable of about 2 × 3 cm. rest of general and systemic examination were unremarkable. On ultrasound examination there was a hypo echoic area of 22 × 30 mm under the skin. It was suspected as stitch granuloma but due to changes observed during menstruation and associated dysmenorrheal it was diagnosed as scar endometrioma. Keeping in view these findings her surgery was performed for excision of the nodule and underlying mass. A 3 × 3 cm nodule was excised from subcutaneous tissue (Figure 2). No sinus or fistulous tract was observed. The nodule was sent for histopathology that confirmed the diagnosis. Patient was put on danazol for treatment of endometriosis and followed up in Gynae OPD regularly. Her symptoms subsided and scar healed. It was a rare case and thus being reported.
Discussion
Scar Endometriosis Is a Rae Condition whose main cause is gynecological/obstetrical sugeries. e.g, in perineum following vaginal delivery with episiotomy. Alternatively, in abdominal scar following cesarean or hysterectomy [5]. Scar endometriosis was also observed in smaller scars as that of laparoscopy or even amniocentesis [6,7]. The condition can be put in differential diagnosis of stitch granuloma, wound hematoma, abscess, dermoid tumor,lipoma ,sarcoma and even malignant tumor. The incidence being rare but case has been seen of malignant transformation of scar granuloma to malignant tumor most commonly clear cell carcinoma if ever happens. The diagnosis is confirmed by histopathology and incidence is 0.5-1% [8]. The condition is best explained as implantation of endometrial tissue in scar [9].
Mainstay of diagnosis is history and examination. Common symptoms are swelling, pain, discharge, bleeding specially during the days of menstruation. Pain and bleeding during menstruation is considered pathognomic of the disease. Ultrasound may aid in diagnosis. Surgical excision is the definitive treatment and final diagnosis is confirmed on histopathology of the excised tissue. Wide excision with 1 cm margin is optimal treatment for larger and recurrent lesions [8,9]. Recurrence is rare though till cases have been reported [10]. Co-existing pelvic endometriosis is also common ranging from 14-24 %. There is a need to rule out pelvic endometriosis and thus long term follow up is required [11,12].
Conclusion
Any presentation after cesarean scar of pain and bleeding more pronounced in menstruation is likely to be scar endometriosis. Although malignant transformation is uncommon, still wide margin excision of the lesion is best treatment option for treatment and prevention of recurrence and malignant transformation.

Figure 1: Nodule on scar line.
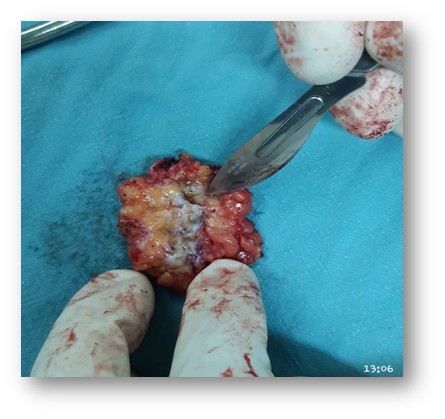
Figure 2: Mass removed per operatively.
Citation: Fatima N, Hashmi KS, Batool S, Shabbir N, Fatima B (2021) Cesarean Scar Sinus Diagnosed as Scar Endometriosis. A Case Report. J Obstet Gynecol Probl: JOGP 100019
