
Annals of Medical & Surgical Case Reports
(ISSN: 2652-4414)
Image Article
Esophageal Achalasia
Ping Huang1,2, Yuan Lu1,2, Wei Liu*1,2
1Institute of Digestive Disease, China Three Gorges University, Yichang, China
2Department of Gastroenterology, Yichang Central People’s Hospital, Yichang, China
*Corresponding Author: Wei Liu, Institute of Digestive Disease, China Three Gorges University, 8 Daxue Road, Yichang 443000, China
Citation: Huang P, Lu Y, Liu W (2020) Esophageal Achalasia. Ann Med & Surg Case Rep: AMSCR-100081
Received date: 12 December 2020; Accepted date: 23 December 2020; Published date: 29 December 2020
A 64-year-old manpresented to the gastroenterology clinic with regurgitation and dysphagia which occurred with every meal, accompanied with postprandial chest pain. For 5 years, he had had difficulty in swallowing both solids and liquids with the symptomworsened during this two months before presentation. Meanwhile, a weight loss of 10 kg was notable in the previous year. Gastroscopy was notable for a detained mass in the esophagus (Figure A) and a tight gastroesophageal junction. Furthermore, a barium esophagram showed esophagram with typical bird-beak appearance of distal esophagus (Figure B). High-resolution esophageal manometry revealed an elevated integrated relaxation pressure of the lower esophageal sphincter and absence of peristalsis, which were consistent with type I (classic) achalasia. The diagnosis of esophageal achalasia was made. Achalasia is considered to be a primary motor disorder of the esophagus,which is characterized by loss of esophageal peristalsis and insufficient lower esophageal sphincter relaxation [1, 2]. This leads to patients’ complaints of regurgitation and dysphagia to liquids and solids, often along with chest pain and weight loss [3, 4]. Appropriate diagnostic and therapeutic strategies should be prompted when endoscopic finds retained saliva with puckered gastroesophageal junction or barium swallow shows dilated esophagus with birds beaking in a symptomatic patient [5, 6]. The patient opted for treatment with peroral endoscopic myotomy (POEM). At follow-up 1year after treatment, he had no dysphagia and regurgitation.
Acknowledgements
Funding: This work was supported by National Natural Science Foundation of China (31600134).
Conflicts of Interest: The authors have no conflicts of interest to declare.
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Written informed consent was obtained from the patient for publication of this “Image”.
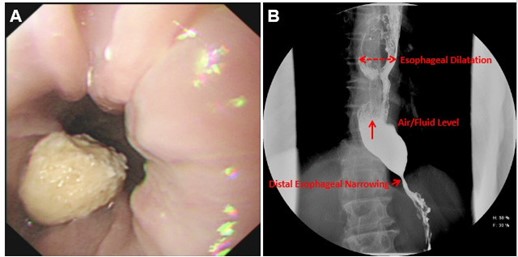
Figure 1: Esophageal achalasia. (A) Endoscopic view of a detained mass in the esophagus. (B) Esophagram with typical bird-beak appearance of distal esophagus;
Citation: Huang P, Lu Y, Liu W (2020) Esophageal Achalasia. Ann Med & Surg Case Rep: AMSCR-100081
