
Annals of Medical & Surgical Case Reports
(ISSN: 2652-4414)
Image Article
Crohn’s Disease Presenting Stenosis of Sigmoid Colon
Ting-Ting Zhou1,2, Li-Min Zheng1,2, Wei Liu*1,2
1Institute of Digestive Disease, China Three Gorges University, Yichang, China
2Department of Gastroenterology, Yichang Central People’s Hospital, Yichang, China
*Corresponding Author: Wei Liu, Institute of Digestive Disease, China Three Gorges University, 8 Daxue Road, Yichang 443000, China
Citation: Zhou TT, Zheng LM, Liu W (2020) Crohn’s Disease Presenting Stenosis of Sigmoid Colon. Ann Med & Surg Case Rep: AMSCR-100080
Received date: 12 December 2020; Accepted date: 23 December 2020; Published date: 29 December 2020
A 15-year-old boy was transferred to our hospital with abdominal pain and vomiting that had progressed over the preceding 2 days. He had presented to the local community hospital with a 1-week history of fever before presentation. He was stunted with both height and weight below the normal level. Physical examination revealed normal vital signs and mild left lower quadrant abdominal tenderness with active bowel sounds. Radiography of abdomen confirmed some air-fluid levels (Figure A). Computed tomography of the abdomen revealed stenosis of sigmoid colon (Figure B). Colonoscopy revealed multiple polyps of stenosis of sigmoid colon and thickening of the wall of the terminal ileum (Figure C), but findings on biopsy of polyps and colonic mucosa were of no clinical value. Considering the potentially associated lesions in the jejunum and ileum, peroral double-balloon enteroscopy was assessed and confirmed numerous ulcers, and the specimen revealed longitudinal ulcers. Crohn’s Disease (CD) were considered to be the most plausible explanation, but the differential diagnosis of the ileum lesions also consisted of tuberculosis, ulcerative colitis and lymphoma. Direct microbiologic detection and cultures were negative for tuberculosis and the human immunodeficiency virus. Pathological examination revealed CD complicated by stenosis of the sigmoid colon. A diagnosis of CD with stenosis of sigmoid colon was made. CD may result from a complex interplay between genetic susceptibility, altered gut microbiota and environmental factors, resulting in dysregulated immune responses [1, 2]. The prevalence of CD is significantly increasing in childrenand adults [3]. The typical clinical feature is a young patient presenting with abdominal pain, fever, weight loss, diarrhoea and fatigue [4, 5]. It is characterized by transmural and patchy lesions which may affect the entire gastrointestinal tract, from the mouth to the anus [6]. CD presenting as an acute abdomen due to colonic obstruction is uncommon [7, 8]. Stenosis of the sigmoid colon in CD is rare [9]. Therapeutic schedules are guided by disease severity and risk of poor outcomes [10]. After a well-informed discussion of options for interventions with the patient’s family, the decision was made to pursue infliximab infusions of 5 mg/kg/dose at 0, 2, and 6 weeks and every 8 weeks thereafter. After the procedure, he clinically recovered with continuous treatment.
Acknowledgements
Funding: This work was supported by National Natural Science Foundation of China (31600134).
Conflicts of Interest: The authors have no conflicts of interest to declare.
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Written informed consent was obtained from the patient for publication of this “Images in Clinical Medicine”.
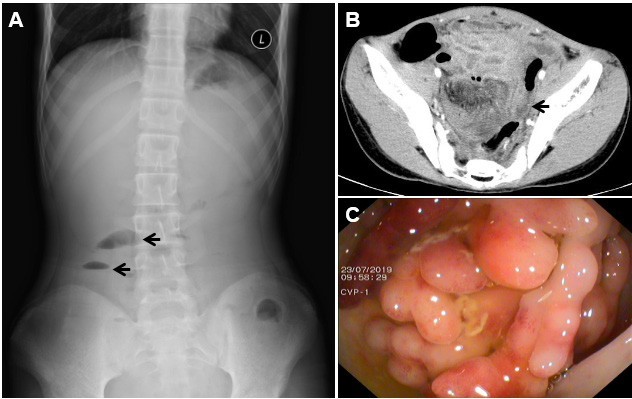
Figure 1: Crohn’s disease presenting stenosis of sigmoid colon. (A) Radiography of abdomen of air-fluid levels (arrows); (B) axial CT image of stenosis of sigmoid colon (arrow); (C) multiple polyps of stenosis of sigmoid colon by colonoscopy
Citation: Zhou TT, Zheng LM, Liu W (2020) Crohn’s Disease Presenting Stenosis of Sigmoid Colon. Ann Med & Surg Case Rep: AMSCR-100080
