
Annals of Medical & Surgical Case Reports
ISSN: 2652-4414
Image Article
Chronic Alcoholic Pancreatitis
Ting-Ting Zhou1,2, Yuan Lu1,2, Wei Liu*1,2
1Institute of Digestive Disease, China Three Gorges University, Yichang, China
2Department of Gastroenterology, Yichang Central People’s Hospital, Yichang, China
*Corresponding Author: Wei Liu, Institute of Digestive Disease, China Three Gorges University, 8 Daxue Road, Yichang 443000, China
Citation: Zhou TT, Lu Y, Liu W (2020) Chronic Alcoholic Pancreatitis. Ann Med & Surg Case Rep: AMSCR-100079
Received date: 12 December 2020; Accepted date: 23 December 2020; Published date: 29 December 2020
A 54-year-old man presented to the outpatient clinic with a 5-year history of abdominal pain and weight loss. Except for alcohol abuse, he had no documented medical history. Physical examination revealed normal vital signs and mild left upper quadrant abdominal tenderness with normal bowel sounds.Laboratory test revealed anormal serum amylase level. Contrast-enhanced computed tomography of the abdomen revealedheavy calcifications of pancreatic head (Figure 1A). Endoscopic ultrasound scan showeda severely dilated pancreatic duct in the head of pancreas (Figure 1B). Considering the ill-defined morphological changes of pancreas in this patient, Three-dimensional magnetic resonance cholangiopancreatography (MRCP) confirmed a minimally dilated biliary tree, pseudocysts of the pancreatic head, and severely dilated irregular main pancreatic duct with calculus in the atrophic pancreas (Figure 2A). The diagnosis of chronic pancreatitis (CP) depended on the typically characteristic endoscopic and MRCP manifestations and was confirmed by pathological examination. CP is considered to be a progressive fibroinflammatory disease often with dilated irregular pancreatic duct and intraductal calculi [1-3]. Alcohol abuse, smoking, and genetic predisposition are the potential risk factors for CP [4-6]. Treatment options include medical, radiological, endoscopic and surgical interventions, and a multidisciplinary approach is necessary [7-9]. After a well-informed discussion of options for interventions with the patient’s family, the decision was made not to pursue pancreatic sphincterotomy and stent placement. He was charged home with clinical symptomatic relief.
Acknowledgements
Funding: This work was supported by National Natural Science Foundation of China (31600134).
Conflicts of Interest: The authors have no conflicts of interest to declare.
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Written informed consent was obtained from the patient for publication of this “Images in Clinical Medicine”.
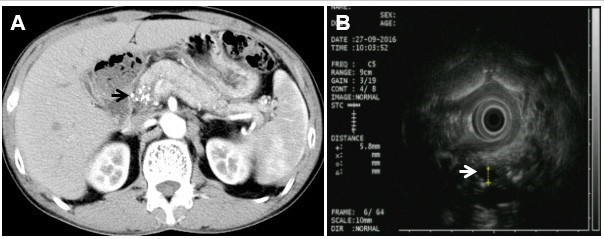
Figure 1: Chronic alcoholic pancreatitis. (A) Contrast-enhanced CT showing heavy calcifications in the pancreatic head (arrow); (B) Endoscopic ultrasound scan shows a severely dilated pancreatic duct in the head of pancreas (arrowed) consistent with severe chronic pancreatitis.
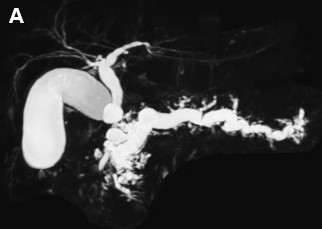
Figure 2: Chronic alcoholic pancreatitis. (A) Three-dimensional magnetic resonance cholangiopancreatogram shows a minimally dilated biliary tree and severely dilated irregular main pancreatic duct.
Citation: Zhou TT, Lu Y, Liu W (2020) Chronic Alcoholic Pancreatitis. Ann Med & Surg Case Rep: AMSCR-100079
