
Emergency Medicine and Trauma Care Journal
(ISSN: 2652-4422)
Lyme Carditis Associated with Complete Heart Block and Cardiac Arrest
Case Report
Ana-Maria Popa and Naqibullah Mirzada*
Department of Clinical Medicine/Cardiology, Nykoebing Falster Hospital, Denmark
*Corresponding author: Naqibullah Mirzada, Department of Clinical Medicine/Cardiology, Nykoebing Falster Hospital, Region Sjaelland, Denmark
Citation: Popa A-M and Mirzada N (2020) Lyme Carditis Associated with Complete Heart Block and Cardiac Arrest. Emerg Med Trauma. EMTCJ-100052
Received Date: 19 September, 2020; Accepted Date: 23 October, 2020; Published Date: 30 October, 2020
Abstract
Lyme Disease (LD), is common and appears as predominantly cutaneous, articular, cardiac and neuro-psychiatric manifestations. Carditis is an uncommon presentation of the early disseminated phase of Lyme disease. LD affects all layers of the heart and every part of the conducting system. Carditis is a less common manifestation of LD. Total heart block has been rarely reported in LD. We present the case of a 73 years male patient who presented with erythema migrans and was found to have first-degree heart block which progressed to complete heart block and asystole within hours.
Case Summary: A 73-years-old male with no previous cardiac claims, was admitted to the emergency department after experiencing two episodes of abrupt syncope. The patient had positive history for tick bite 14 days prior to admission and erythema migrans on the abdomen. Initial ECG showed first degree AV block and right bundle branch block, which progressed within hours to third degree AV block, followed by ventricular asystole and circulatory collapse. After successful resuscitation, a permanent pacemaker was implanted due to the severity heart block, along with the standard antibiotic therapy.
Conclusions: Manifestations of Lyme Carditis (LC) vary from asymptomatic and symptomatic electrocardiographic changes and Heart Block (HB) can occur with potential risk for sudden death. Lyme carditis should be suspected in individuals with cardiac manifestations in an endemic area. Our case illustrates the importance of early recognition and anticipation of progressive cardiac conduction abnormalities in patients presenting with Lyme disease.
Keywords: Borrelia burgdorferi; Heart block; Lyme carditis; Lyme disease; Tick(s)
Background
Lyme Disease (LD), is common in Europe, with predominantly cutaneous, articular, neuro-psychiatric and cardiac manifestations. The incidence of Borreliosis in Denmark is not known, presumably a few thousand people are infected every year. In most cases, it is a localized infection of the skin. Seroprevalence among blood donors in Europe ranges from about 2% in Denmark up to about 10% in high endemic areas. At risk groups such as foresters and farmers and in high-endemic areas, up to 40% can be seropositive. Lyme carditis is reported to occur in 0.3-4% of untreated European patients with erythema migrans [1]. The diagnosis is rarely made. Rare case of Lyme Carditis (LC) have been reported and the incidence of LC in patients with LD varies from 0.2-10% in different reports [2-4]. LC may present with or without other manifestations of LD and could involve all layers of the heart: myocardium, pericardium, endocardium [4-14]. Cardiac involvement is typically seen weeks to months (7 days - 7 months) after a tick bite. Any part of the conducting system could be affected, and conduction blocks of varying degrees may occur. ECG changes in LD can occurs up to 29% [15].
Case Presentation
A 73-years-old male with past medical history of significant for lever cirrhosis and hepatitis C. No previous cardiac claims presented to our emergency department after experiencing two episodes of abrupt syncope. 14 days prior to the ER admission, while working in the garden, he remarked a tick bite on his abdomen, which continued to expand in size the following days. He did not seek medical attention at that time. Physical exam was unremarkable except a 15x15 cm annular rash on the abdomen (Figure 1). Laboratory findings on admission inclusive troponin were within normal. Further workup included a normal lumbar puncture and a normal echocardiography. Lyme serology (Borrelia IgG) was highly positive.
Borrelia IgG = 102,30. Initial ECG on admission reveled first degree AV block and right bundle branch block (Figure 2). After a few hours in the ER department, the patient developed intermittent third-degree AV block, followed by ventricular asystole and circulation collapse (Figure 3). Successfully resuscitated and treated with atropine, isoprenaline and extern pacing. A temporary pacemaker has been implanted, followed by a permanent pacemaker. The decision of permanent PM made by consensus due to severity of heart block causing in-hospital asystole. He was discharged and continued with per oral doxycycline course after initial 7 days of intravenous penicillin. The follow-up 3 months PM control was unremarkable.
Discussions and Conclusions
Carditis is an uncommon manifestation of disseminated Lyme disease, and third-degree AV block is rarer still. Nevertheless, third-degree AV block can result in fatal arrhythmias if not managed and treated appropriately. AV block associated with Lyme carditis is due to effects of the host inflammatory response directed at the spirochetes in cardiac tissue. The most common clinical manifestation is Atrioventricular (AV) conduction blockade, which can fluctuate rapidly and progress from first- to third-degree heart block within minutes to hours [17]. The average time from initial presentation to complete heart block is 2 weeks (2-24 days). The time for resolution of complete heart block, after treatment is initiated, is usually 6 days although it can vary from 1 day to 7 weeks [18]. In our case, the initial skin rash occurred few days after the thick bite and cardiac symptoms with syncope and complete heart block occurred first at 2 weeks following the tick bite.
Clinical features such as tick bite, erythema migrans, arthritis, typically provide strong diagnostic evidence of Lyme involvement, but primary conduction system disease without evidence of tick bite or rash can make the diagnosis challenging. Therefore, basic investigations including the history of possible tick exposure, laboratory testing, a 12-channel electrocardiogram, and in hospital continuous ECG monitoring, chest x-ray, echocardiography and check of labs inclusive Lyme serologi is highly recommended in patient from endemic areas presenting with erythema migrans and/or with symptoms such as pre-syncope, syncope, worsening shortness of breath, or chest pain with are suggestive of cardiac involvement [18]. Although extern pacing is mainly used in LC patients as a supportive treatment until the antibiotic course is finished and the heart block is resolved, permanent PM implantation in patients with LC and recurrent CHB with asystole should be considered by consensus. Furthermore studies on this issue is needed.
Consent
Informed consent for the publication of this paper has been obtained and is available on request. All patient identifiers have been removed to ensure patient’s privacy.
Competing Interest
The authors declare that there is no conflict of interest regarding the publication of this paper.
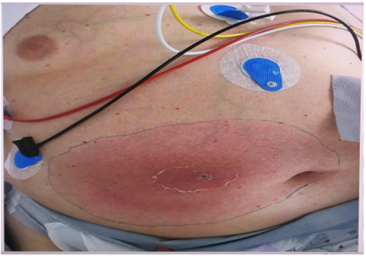
Figure 1: Physical exam was unremarkable except a 15x15 cm annular rash on the abdomen.
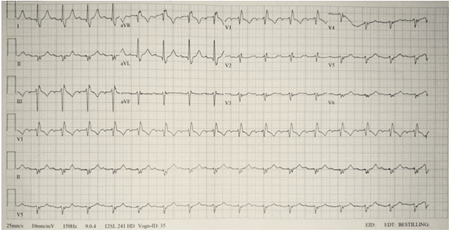
Figure 2: Initial ECG on admission reveled first degree AV block and right bundle branch block.
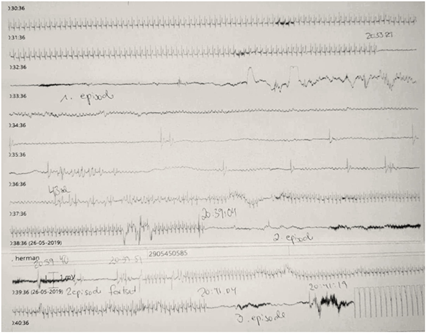
Figure 3: ER department, the patient developed intermittent third-degree AV block, followed by ventricular asystole and circulation collapse.
Citation: Popa A-M and Mirzada N (2020) Lyme Carditis Associated with Complete Heart Block and Cardiac Arrest. Emerg Med Trauma. EMTCJ-100052
