
Annals of Medical and Surgical Case Reports
ISSN: 2652-4414
The Effect of Nail Diameter and Size of Bone Defect on Strength and Stiffness of a Composite Femur - Titanium Intramedullary Nail Construct
Anthony Howard1*, Marlow W2, Panteli M1, McLauchlan G3
1Academic Department of Orthopaedic Surgery, Leeds University, England
2Royal Liverpool Hospital, England
3Royal Preston Hospital, England
*Corresponding author: Anthony Howard, Academic Department of Orthopaedic Surgery, Leeds University, Leeds, England
Citation: Howard A, Marlow W, Panteli M, Mc Lauchlan G, (2020) The Effect of Nail Diameter and Size of Bone Defect on Strength and Stiffness of a Composite Femur - Titanium Intramedullary Nail Construct. Ann Med &Surg Case Rep: AMSCR-100072
Received Date: 09 October, 2020; Accepted Date: 23 October, 2020; Published Date: 30 October, 2020
The study aimed to determine the effects of intramedullary nail diameter and size of bone defect in comminuted fractures on strength and stiffness of a composite femur - Stryker T2 Femoral Nail construct.14 Stryker T2 Femoral Nails of diameters 10mm, 11mm and 13mm were inserted into fourth generation composite femurs. A 3cm osteotomy gap was created mid femoral shaft. Axial compression was measured. Stress-strain patterns were analysed and strain at 1500N was compared between different diameter nails using one-way ANOVA analysis. The osteotomy gap was then increased in steps to 5cm, 8cm and 10cm.
The strain at 1500N was compared between osteotomy gaps using repeated measures ANOVA pairwise comparison. There was a significant increase in stiffness was noted with increasing diameter (p values <0.012). The 10mm nails all demonstrated plastic deformation below 2000N. An increase in osteotomy gap was demonstrated to cause a trend towards reduced stiffness of the construct - this was significant in the 5cm vs. 8cm comparison (p = 0.044).The worked showed that 10mm Stryker T2 femoral nails used in comminuted fractures should not be weight bearing until the fracture is united. Increasing osteotomy gap may reduce stiffness of the construct.
Introduction
Intramedullary fixation is the gold standard for stabilisation of adult femoral diaphyseal fracture [1,2]. The key biomechanical advantages of intramedullary fixation over the use of a plate are a reduced lever-arm distance and load-sharing with cortical bone. In segmental or comminuted fractures, the latter advantage is removed - in this situation, the device becomes load-bearing. Designs of femoral nails have varied since their introduction of a steel clover-leaf nail by Küntscher in 1942. Current vogue favours titanium nails because of their Young’s modulus of elasticity, which is closer to that of bone than steel, and therefore reduces stress shielding. However titanium has its disadvantages in the form of fatigue stress, expense and difficulties in manufacture. Previous studies of biomechanical limits of intramedullary nails have studied steel nails or used non-physiological loading methods in testing nails [3-7]. There have been no previous studies testing the limits of titanium nails in segmental fractures loaded in a physiological manner.
The stiffness of a nail is determined by its material and second moment of area - determined by diameter and cross-sectional pattern. A nail will exhibit elastic deformation under stress until its yield point. When plastic deformation or breakage occurs, the nail is said to have failed. Previous population studies suggest a risk of bending of between 1.5% and 4.3% [8,9]. The purpose of this study was to determine the limits of titanium intramedullary femoral nails of varying diameters within a composite bone when loaded physiologically. This would determine whether nails used in segmental fractures could be weight bearing in the immediate post-op period without risking early failure.The secondary outcome was to assess whether the size of an osteotomy has a significant impact on stiffness of the construct.
Materials and Methods
Fourth generation composite femurs (Sawbones, Pacific Laboratories Inc.) were selected for their mechanical properties replicating real bones [10]. Stryker T2 cannulated titanium nails of varying diameter and length were selected for their common use in clinical practice; four 10mm diameter, five 11mm diameter and five 13mm diameter nails were tested. The femurs were reamed to 2mm above the nail diameter. The nail was inserted into the femur and a proximal locking screw was inserted. One distal interlocking screw was inserted since compression has been shown to be unaffected by the insertion of a second screw [11].A 3cm osteotomy was simulated initially with the distal cut at the mid-shaft of the femur. The construct was then loaded into an electro-hydraulic testing machine. The femoral head was loaded through a hemispherical surface padded with rubber.
The femoral condyles were loaded through a plate mounted on a mobile bearing. These measures reduced the artificial shear forces in order to replicate physiological loading.The construct was then loaded up to 2,100N and load versus axial displacement was measured. 2,100N was chosen since this represents the load of 3 times the bodyweight of an average 70kg adult.Axial force has been shown to generate 2.2-2.5 times bodyweight while walking on the flat and 2.8 times bodyweight when descending stairs [12]. Tests were terminated if the displacement reached 25mm.The next nail of the same diameter was then replaced into the composite bone and the loading repeated. The osteotomy gap was then increased to 5cm, 8cm and then 10cm with the distal cut at the mid-shaft point and the loading repeated for each of the nails.
This process was repeated with a new composite femur for each diameter of nail. The nails and interlocking screws were checked between tests for signs of deformation. One-way ANOVA analysis was used to calculate significance of diameter of nail versus mean axial displacement under a load of 1400N (2 times bodyweight). Gaussian distribution was tested using the Wilk-Shapiro test and variation between groups was shown to be the same using Levene’s test. Repeated measures ANOVA with pair wise comparison was used to determine whether the size of the osteotomy had a significant effect on displacement.Second moment of area of each nail was measured using a micrometer using the equation:
I = π (r4-i4)/4
Results
Load versus displacement for each diameter nail and for each osteotomy size was plotted graphically which demonstrated two phenomena clearly as can be seen in (Figure1). The first is that in some tests there was slippage of the construct - this is demonstrated as a vertical drop in the line as the slip allows dissipation of some of the force (sky blue line in Figure 1). The second is that in some tests the nails reached their yield point before the 2,100N load was reached as can be seen in the flattening of the gradients of the plots in Figure 1. In the 11mm and 13mm diameter nails, the gradient of the plots generally remained constant and this yield point was only reached in one of the 11mm nails which failed at 1,700N (Figure 2).The consequence of the 10mm nails reaching their yield point and becoming plastically deformed was that they could not then be tested with varying size osteotomy.
The mean displacement of the nails at 1,400N at each osteotomy size is demonstrated in Figure 3. This decrease in displacement with wider diameter nails was demonstrated to be significant using one-way ANOVA analysis (Table 1).The mean displacement at 1,400N with each osteotomy size was compared in a pair-wise manner using repeated measures ANOVA comparison (Table 2). This demonstrated a significant increase in displacement with increased osteotomy size in the 5cm versus 8cm osteotomy comparison. This was the only difference which reached significance and this was after exclusion of tests where there had been slippage.The second moment of area of each nail is demonstrated in Table 3.
Discussion
There have been no other studies to determine the load under which cannulated titanium nails of different diameters will fail. In addition there have been no studies considering the effect of the size of the osteotomy on the load at which a nail will fail.The 10mm diameter nails were loaded with a 3cm osteotomy gap. The load displacement plots demonstrate that all four of these nails reached their yield points between 1,300N and 1,800N. An average 70Kg adult will load a between 1,500N and 1,700N while walking on the flat and 1,900N while descending stairs[12]. These figures suggest that patients whose femoral shaft fractures are stabilised using 10mm cannulated titanium nails should not be allowed to fully weight-bear if the fracture configuration is not innately stable.In loading the 11mm nails, only one nail that failed at 1,700N however a slight reduction in the gradient was noted as the remaining four nails approached 2,100N.
This would suggest that patients with an unstable fracture fixed with the 11mm nails could be cautiously mobilised fully weight-bearing immediately post-op with avoidance of activities such as running and descending stairs.Since the 13mm nails did not demonstrate plastic deformation below 2,100N and did not demonstrate flattening of the gradient of their plots as they approached this load, this suggests that patients whose fractures are stabilised with 13mm nails could safely be mobilised fully weight-bearing with a margin of confidence.This reduction in displacement and higher yield point is most likely to be due to the increase in second moment of area with wider diameter nails as is seen in Table 3.The size of the osteotomy showed a small trend towards increased osteotomy size increasing displacement under load; however this was significant in only one case - 5cm versus 8cm osteotomy.
The amount of displacement was not seen to be proportional to the size of the osteotomy. In addition, since the osteotomy was enlarged stepwise proximally, the proximity of the proximal cut to the upper end of the shaft may have introduced a confounding factor. A larger osteotomy presents a larger length of the beam which has a smaller second moment of area - i.e. a nail unsupported by surrounding bone. A larger osteotomy would therefore be expected to be associated with increased bending, however this was not strongly supported by our results.This study is limited by the fact that in vivo the construct would be loaded in a multidirectional manner by muscle pull including forces of shear and rotation. This has been compensated for by using loading points designed to mimic physiological axial loading. In vivo the loading would be cyclical, however this factor was not replicated in the study.
In order to ascertain whether these compromises will bias clinical outcome, it would be necessary to compare rates of failure in patients who are treated with each diameter of titanium femoral.Drill holes placed in the femur for the distal locking screws could have caused a stress riser when a different length nail was then used in the composite femur; however there was no incidence of fracture through these drill holes. In some tests, there was slippage of the construct in the loading platform. This would have increased the apparent displacement for a specific load therefore these tests were omitted when comparing displacement between different osteotomy sizes. Different length nails were used in this study - this may have introduced a confounding factor since the femurs were reamed to 2mm above nail diameter and bending could have occurred within the femoral canal, however, the same selection of nail lengths were compared for each diameter nail so this factor is likely to have been mitigated.
Conclusion
This study demonstrates the clinical limits of cannulated titanium nails of the diameters 10mm, 11mm and 13mm. In segmental fractures, 10mm nails should be avoided since they will not provide sufficient strength to fully weight-bear in a typical adult. 11mm nails could be used in this case with caution, with preference for 13mm nails if the femoral canal allows. The results confirmed the significant effect of diameter on second moment of area, bending stiffness and yield point as would be expected.The expected reduction in bending stiffness with increased osteotomy gap was not significantly verified; however this may be due to confounding by the position of the osteotomy on the femoral shaft. Comparison between constructs with the same size osteotomy at different points along the femoral shaft should be conducted to verify whether this has a clinically relevant impact.
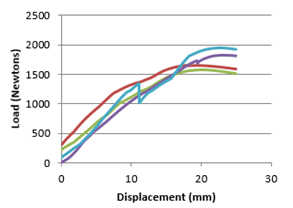
Figure 1: Load versus Displacement plot for a 10mm nails with a 3cm Osteotomy.
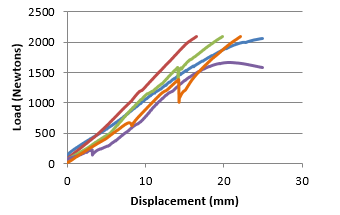
Figure 2: Load versus Displacement plot for an 11mm nails with a 5cm Osteotomy.
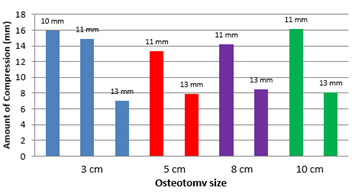
Figure 3: Mean displacement of each size nail at 1,400N at each osteotomy size.
|
Osteotomy Size |
Degrees of Freedom |
F |
Significance (p) |
|
3cm |
2 |
6.373 |
0.012 |
|
5cm |
1 |
35.555 |
0.000 |
|
8cm |
1 |
18.911 |
0.003 |
|
10cm |
1 |
19.738 |
0.003 |
Table 1: One-way ANOVA calculated significance of the affect of diameter of a nail on displacement under a load of 1,400N - calculated for each osteotomy size.
|
Osteotomy sizes compared |
Mean difference in displacement (mm) |
Significance (p) |
|
3cm versus 5cm |
17.87 |
0.5249 |
|
3cm versus 8cm |
-2.34 |
0.925 |
|
3cm versus 10cm |
-9.58 |
0.729 |
|
5cm versus 8cm |
-20.20 |
0.044 |
|
5cm versus 10cm |
-27.45 |
0.088 |
|
8cm versus 10cm |
-7.24 |
0.634 |
Table 2: Repeated measures ANOVA pair-wise comparison of displacement for each osteotomy size under 1,400N load with exclusion of tests where there was slippage.
|
Diameter of Nail (mm) |
Internal Radius (mm) |
External Radius (mm) |
Second Moment of area (mm4) |
|
10 |
2.25 |
5 |
470.74 |
|
11 |
2.33 |
5.5 |
2,782.16 |
|
13 |
2.38 |
6.5 |
5,507.14 |
Table 3: Second Moment of area calculated for each diameter of cannulated nail.
Citation: Howard A, Marlow W, Panteli M, Mc Lauchlan G, (2020) The Effect of Nail Diameter and Size of Bone Defect on Strength and Stiffness of a Composite Femur - Titanium Intramedullary Nail Construct. Ann Med &Surg Case Rep: AMSCR-100072
