
Journal of Urology and Renal Problems
(ISSN 2652-4805)
Case Report
A Systematic Literature Review of Complications Associated with Robotic-Assisted Partial Nephrectomy
Renzulli II JF* and Broccoli I
Department of Urology, Yale School of Medicine, USA
*Corresponding author: Joseph F. Renzulli II, Department of Urology, Yale School of Medicine, USA
Citation:Renzulli II JF and Broccoli I (2020) A Systematic Literature Review of Complications Associated with Robotic-Assisted Partial Nephrectomy. J Urol Ren Probl: JURP-100010
Received date: 07 August, 2020; Accepted date: 25 August, 2020; Published date: 31 August, 2020
Abstract
Objectives: To determine the most common complications associated with robotic-assisted partial nephrectomy (RAPN), the incidence of occurrence and the recommended treatment approach to each complication.
Patients and Methods: Peer review articles containing their own data collected between April 1994 and April 2020 were used to determine the types and severity of complications associated with RAPN. We reviewed 53 papers and included 28 papers that met criteria.
Results: Patients from each study reporting complications were included in the analysis. The overall rate of complications across the 28 studies was 18.3%. The most common complications were hemorrhage, urine leaks, renal failure, and pseudoaneurysms. Age, tumor size, and weight had little to no effect on patient complications, although operating time and warm ischemia time were crucial factors. Complications were ranked based on the Clavien-Dindo classification. No complications achieved higher than a IV ranking. No deaths occurred throughout the 28 studies. Appropriate interventions to address the complications were included in our review if the study presented them.
Conclusion: RAPN is a successful but advanced robotic procedure to address renal masses. However, there are a significant amount of complications that can be encountered. Surgeons must be aware of these complications and know the proper protocol for addressing each one. Due to the potential complications with RAPN, we sought to review the literature and quantify the complications associated with RAPN.
Keywords: kidney; Renal mass; Renal carcinoma; Serum; Surgery
Case Report
A 56-year-old male with a 3cm right lower pole, partially endophytic, renal mass underwent a robotic assisted partial nephrectomy. The patient had an uneventful procedure and was discharged post -operative day 2. The patient developed right flank pain 10 days’ post procedure and some minor hematuria. A CT scan revealed that he had a large perinephric collection. The collection of fluid extended to above the liver. A perinephric drain was placed within the collection and the fluid was tested for creatinine and it was elevated above serum levels consistent with urine. A retrograde pyelogram revealed a small calyceal leak at the site of the partial nephrectomy repair site. Therefore, a double J ureteral stent was also placed. Once the drainage was less than 1 ounce per day, the patient’s drain creatinine level was rechecked and was consistent with serum. A CT scan confirmed resolution of the perinephric collection. The drain was removed. The ureteral stent was left in place for six weeks, and then another retrograde pyelogram was performed in the operating room and revealed no extravasation. The stent was removed, and the patient has fully recovered. Pathology confirmed a clear cell renal carcinoma with negative margins.
Introduction
In 2019, more than 73,000 people in the United States will be diagnosed with kidney cancer[1]. A partial nephrectomy is performed to remove a tumor, often cancerous, from a kidney. Radical nephrectomy or partial nephrectomy are the two most commonly offered procedures for a patient presenting with a renal mass. The surgeon may recommend that the patient have either an open surgery or robotic/laparoscopic surgery depending on multiple factors. Robotic surgery has surgeons to perform complex dissection and suturing to be done with significant ease compared to pure laparoscopy and therefore, has become the standard of care to address small renal masses [2].
RAPN has become the standard method of surgery for patients with kidney tumors less than 4cm (T1a). Tumors up to 7cm (T1b) can be considered if located in certain areas of the kidney. To start the procedure, a small incision is created in the abdomen where a camera and robotic surgical instruments can be inserted. The kidney is identified and the vascular structures supplying the kidney are dissected. The hilar vessels are clamped with laparoscopic clamps to temporarily stop blood flow to the kidney, and then removal of the cancerous portion from the kidney commences [3]. The robotic platform helps to provide 3-D images during the procedure and can make complex movements easier for the surgeon. Studies have evaluated open versus laparoscopic versus robotic nephrectomy outcomes and essentially the robotic technique is either equivalent or superior in all evaluated categories [4,5].In most cases, RAPN is preferred over open partial nephrectomy (OPN) and laparoscopic partial nephrectomy (LPN) due to fewer complications, making it the safest procedure [6].
Complications related to RAPN can be significant and the care team must be aware of the signs and symptoms related to these complications. The complication rate in RAPN can be as high as 18.3%, and each of these complications are ranked by the Clavien-Dindo system[7]. This system helps categorize the complications to standardize them across hospital systems, regions, and surgeons. It allows for a better perspective of how significant a complication is related to another complication. Once a complication arises, the surgeon must know how to successfully manage the issue. The vast number of complications associated with RAPN can be easily resolved if identified in a timely manner.
Materials and Methods
We performed a systematic literature search on google scholar evaluating peer review articles for RAPN. The search was done in June of 2020 and was performed by searching for articles consisting of “robotic assisted partial nephrectomy”, “complications”, and “disadvantages”. All the studies included were completed between April 1994 and April 2020. Papers comparing RAPN, LPN, and OPN were also included. Articles describing management methods for complications of partial nephrectomy were included. Medical complications were excluded. We assessed 28 papers that met our inclusion criteria.
Results
Table 1shows the baseline characteristics of the average patient gathered from each study. Each study had mean patient characteristics that were then compared to data from other studies to determine the overall mean. Not all peer review articles displayedthese characteristics. The mean age range across all trials was 55-66 years. The mean tumor size range across trials was 2.6-3.9 cm. More importantly, warm ischemia time and operating time were principal factors relating to complications. Warm ischemia time is preferred to be under 30 minutes. The average ischemic time across studies was 21.2 minutes. The mean warm ischemia time range across all trials was 13-31.6 minutes. Meanwhile the mean operating time range was 90-255 minutes, which represents a significant variance.
Complications associated with robotic-assisted partial nephrectomy were searched and recorded through a series of studies, and an average percentage of each complication was recorded in Table 2. After collecting the percentage of each specific complication from the articles that contained them, these percentages were averaged together to get a better understanding of how frequent these complications occur.
Figure 1 compares each averaged complication type. Complications occur about 18.3% of the time, with most of those being postoperative complications (13%). Hemorrhaging is common in patients; Intraoperative, postoperative, and delayed hemorrhaging all together happens about 10.7% of the time. Pseudoaneurysms occur about 10.9% of the time, and postoperative ileus occurs 3.3% of the time.
Table 3 shows the Clavien-Dindo classification along with the average percentage of complications occurring in each range of the classification. To correct a specific complication, the complication is ranked by the Clavien-Dindo classification on how severe it may be to a patient. There are seven grades within five categories (I, II, IIIa, IIIb, IVa, IVb, and V), where I is the lowest ranked severity complication and V is the highest. In the articles that mentioned the Clavien-Dindo classification for complications observed, the average percentage of each range of grade was recordedand calculated. About 25.3% of complications that occurred throughout these peer review articles were under the grades I and II. Between III and IV there are four grades (including their sub grades), and these had a rate of 7.7% of complications. Grade V was not observed in any of the studies.
Figure 2 displays the average percentage of complications based on the Clavien-Dindo classification. Complications on the Clavien-Dindo scale were taken from a series of peer review articles and averaged to get a precise percentage. These percentages are shown on a pie chart to get a better understanding of the range and severity of complications that occur during RAPN.
Table 4 shows repair mechanisms for complications that occur during robotic assisted partial nephrectomy and their average percentage of when they occurred throughout the examined peer review articles. Not all peer review articles examined repair mechanisms. The largest types of repair methods were collecting system repair (35%) and calyceal repair (52.1%). Perioperative blood transfusion was also common, at 5.6%.
Discussion
This review sought to evaluate the various complications related to robotic assisted partial nephrectomy and their occurrence rate. Complications associated with partial nephrectomy occur in approximately 1 in 5 procedures. The average percentage of complications resulting from RAPN from all studies reviewed was 18.3%. This incidence is considered high especially since this is the most common procedure performed for small renal masses today. Intraoperative complications are less frequent than postoperative complications, with an incidence of 3.1% and 13%, respectively. One study reviewed 347 patients who underwent a robotic assisted partial nephrectomy. The overall complication rate was 14.7%; intraoperative complications were observed in 2.9% and postoperative in 11.8% [8-15]. Hemorrhage was one of the most common complications observed. Throughout the discovered data, intraoperative hemorrhaging occurred an average of 2.5% of the time, postoperative occurred 4.3%, and delayed occurred 3.9%. state that intraoperative hemorrhaging occurred in 1% of patients, and postoperative in 5.8% in their study consisting of 886 patients [9]. Urine leaks were not as common but there were reports in some cases. A study consisting of 395 patients who underwent a RAPN had an overall incidence of 0.25% for urine leaks [10]. Urine leakage was observed in a couple of articles and had an average occurrence of 1.6%. The average percentage of occurrence for pseudo aneurysms was 10.9% describes a study involving 998 patients, 1.7% of which had pseudo aneurysm[11]. These specific complications were the ones with the highest reporting patient number.
The Clavien-Dindo classification is the best way to gauge how severe complications are. Only a few articles acknowledged the system. One of these articles classified 76.1% of cases into grades I-II and 23.9% of cases into grades III-IV [12-20]. In general, 77% of complications fell into the range of grades I-II and 23% were grades III-IV. There were no cases reporting a grade V complication.
Repair mechanisms were accounted for in several studies. The most prominent being collecting system repair, which was mentioned only in one study involving 998 patients. Of these patients, 35% required collecting system repaired [11]. Perioperative blood transfusion was required in multiple trials. A study including 14,275 patients had a blood transfusion rate of 6.2% of the time. Altogether, blood transfusions averaged a 5.6% occurrence [13,21-29]. Calyceal repair was also only mentioned once, but the number was significant reported that a study performed for 183 patients had a rate of 52.1% of patients who required calyceal repair [14, 30-33]. It should be noted that when calyceal repair is required, the percentage for urine leak increases.
Conclusion
The data presented in these peer reviewed articles were reliable and necessary for patients to understand more about robotic assisted partial nephrectomy and appropriately counsel patients who are contemplating the surgery. Although complications remain a major concern, RAPN is proven to be an excellent approach with excellent oncologic outcomes. RAPN is the preferred surgery method over LPN and OPN since there are fewer complications reported. All surgeons should know the signs and symptoms of the complications of RAPN and how to manage these complications if and when they arise.
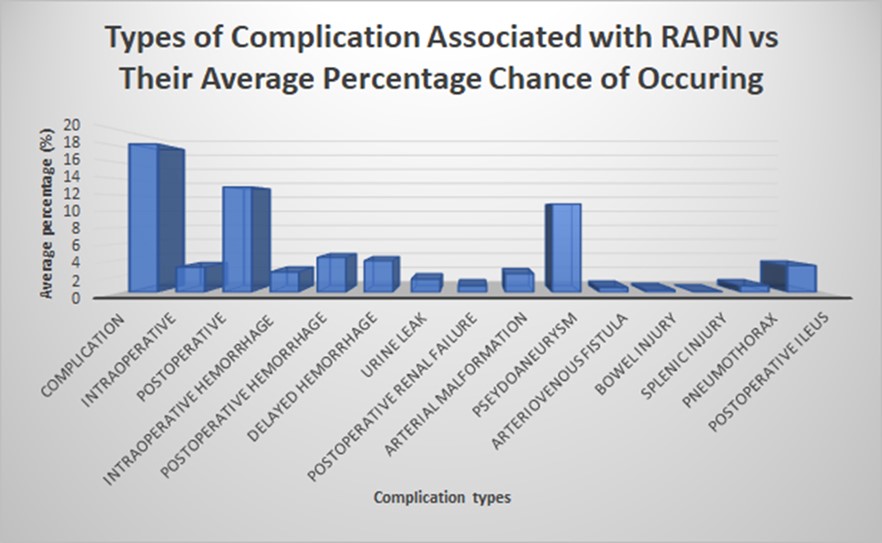
Figure 1:Average percentage of occurrence for each complication type correlated to RAPN.
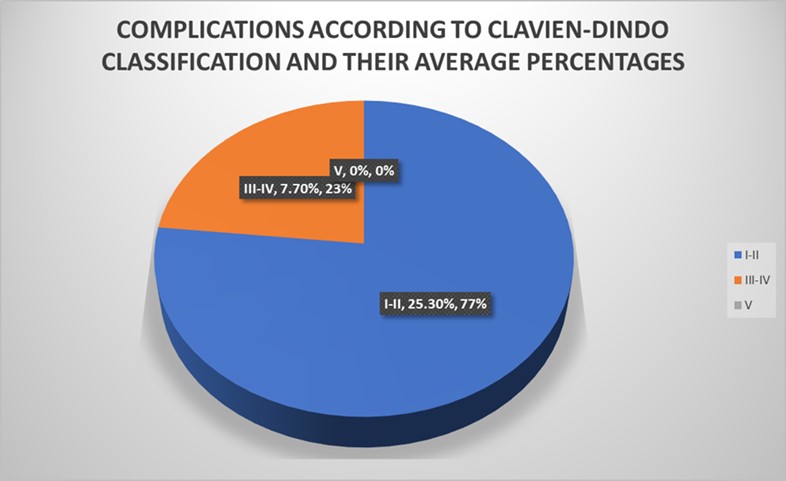
Figure 2:Complications according to the Clavien-Dindo classification system.
|
Characteristics |
Mean |
|
Age |
60 years |
|
Tumor Size |
3.2 cm |
|
Weight |
34.9 kg/m2 |
|
Operating time |
175.8 minutes |
|
Hospital stay |
3.2 days |
|
Warm ischemia time |
21.2 min |
|
Blood Loss |
206.07 mL |
Table 1:Patient mean baseline characteristics.
|
Complication Type |
Average percentage when complication occurs |
|
Overall Complications |
18.3% |
|
Intraoperative |
3.1% |
|
Postoperative |
13% |
|
Hemorrhage intraoperative |
2.5% |
|
Hemorrhage postoperative |
4.3% |
|
Hemorrhage (delayed) |
3.9% |
|
Urine leak |
1.6% |
|
Postoperative renal failure |
0.8% |
|
Arterial malformation |
2.3% |
|
Pseudoaneurysm |
10.9% |
|
Arteriovenous fistula |
0.6% |
|
Bowel injury |
0.3% |
|
Splenic injury |
0.1% |
|
Pneumothorax |
0.8% |
|
Postoperative ileus |
3.3% |
Table 2:Average percentage of occurrence for each complication related to RAPN.
|
Clavien-dindo classification |
Average percentage of complications |
|
I-II |
25.3% |
|
III-IV |
7.7% |
|
V |
0% |
Table 3:Clavien-Dindo classification on the scale of I-V for average percentage of complications related to RAPN.
|
Repair mechanisms |
Average percentage when occurred |
|
Collecting system repair |
35% |
|
Perioperative blood transfusion |
5.6% |
|
Angioembolization |
1.7% |
|
Hemodialysis |
0.2% |
|
Surgical re-exploration |
0.2% |
|
Ureteral stenting |
0.3% |
|
Percutaneous drainage |
0.2% |
|
Calyceal repair |
52.1% |
Table 4:Average percentage of repair mechanisms occurring after RAPN.
Citation:Renzulli II JF and Broccoli I (2020) A Systematic Literature Review of Complications Associated with Robotic-Assisted Partial Nephrectomy. J Urol Ren Probl: JURP-10001
