
Journal of Surgery and Insights
ISSN 2652-4643
Research Article
Gastrointestinal Pathologies in a Center with Limited Resources: Pilot Study at Bafoussam Regional Hospital, Cameroon
Enow Orock G1, 2*, Enow Orock A2, Ngounou E2, Konang N Jl2, Noubom M3, Nzeukou E1, Tabeu Nm1 and Luma H4
1Department of Pathological Anatomy and Cytology, Bafoussam Regional Hospital, Cameroon
2Department of Biomedical Sciences, University of Buea, Cameroon
2Department of Gastroenterology, Bafoussam Regional Hospital, Cameroon
3Department of Medical Biology, Bafoussam Regional Hospital, Cameroon
4Department of Gastroenterology, General Hospital Douala, Cameroon
*Corresponding author :Enow Orock G, Department of Pathological Anatomy and Cytology, Bafoussam Regional Hospital, Cameroon.
Citation: Enow Orock G, Enow Orock A, Ngounou E, Konang N Jl, Noubom M, et al. (2020) Gastrointestinal Pathologies in a Center with Limited Resources: Pilot Study at Bafoussam Regional Hospital, Cameroon. J Surg Insights: JSI-100022
Received date: 23 July, 2020; Accepted date: 27 July, 2020; Published date: 03 August, 2020
Abstract
Aim: Pathology of the digestive tract is common in Cameroon. Despite this situation, studies of gastrointestinal pathology are rare. The pathological anatomy service is almost non-existent in the Cameroonian suburbs. Bafoussam in the west of the country is a semi-urban area and one of the rare ones to have a pathological anatomy department. This is why we have decided to present the epidemiological data of the pathologies of the digestive tract of thislocality.
Méthods: We conducted a three-month prospective study (October 2019-January 2020), in the pathological anatomy department of the Bafoussam Regional Hospital in Cameroon with the aim of presenting the structural pathologies of the digestive tract listed in this institution.
Results: The pathology of the digestive tract has an incidence of approximately 400 in this locality, and represents 45.24% of all the pathologies identified in the pathological anatomy service of the Bafoussam Regional Hospital The age of our patients varies between 17 and 98 years old, with an average of 52.8. Women are slightly more represented (sex ratio M: F of 1: 1.3). Samples from the digestive tract represent 45% of all histological samples recorded in this department. The most common location, in decreasing order, is the stomach (84%), followed by the esophagus (5%), the colon and the rectum (4% each). On the other hand, other sites including the duodenum are rather rare. Of 100 digestive tract samples examined, 98 were pathological with a preponderance of inflammatory lesions (80.61%) against 19.39% of neoplastic nature. The inflammatory pathology was distributed uniformly in all age groups while the malignant pathologies were not observed until after 50 years. Malignant pathologies were more common in men (sex ratio M: F of 3: 1). Gastritis was the most common diagnosis (76.53%) and 94.66% of these gastritis were associated with Helicobacter pylori.
Conclusion: The pathology of the digestive tract is important in our community and dominated by the inflammatory type. The most common site is the stomach, most of the damage to which is caused by Helicobacter pylori. It would be desirable to actively seek out and eradicate Helicobacter pylori infection to decrease the incidence of digestive pathology. Further studies are recommended to establish the true epidemiologic trend of gastrointestinal pathology in our community.
Keywords: Bafoussam; Cameroon; Digestive; Pathology
Introduction
The gastrointestinal tract (IGT) is one of the most complex devices in the body because it has to perform several functions, including digestion and absorption of nutrients. Exposed to a continuous insult from the local macrobiota, the latter' sepithelium is constantly renewed [1]. Several pathological conditions can thus affect the TGI.
Digestive diseases affect millions of patients around the world with a significant economic impact including high cost of the healthcare system, absenteeism at work, and poor quality of life in patients [2-4].
Studies report that gastrointestinal pathology is common in Cameroon [5]. Another indicates that these pathologies constitute 10% of the problems of patients in consultation in the regional hospital of Limbe and at the regional hospital of Buea, in the southwest region of Cameroon [6]. Studies on histologically confirmed structural gastrointestinal pathology are rare in Cameroon and little done in tropical environments [7,8]. This scarcity is attributed to a lack of anatomy-pathological services in Cameroon. This work presents an overview of structural pathologies of the gastrointestinal tract in our community.
Materials and Methods
We conducted a prospective study over a period of 03 months (October 2019 - January 2020). The study concerned surgical specimens sent to the pathological anatomy laboratory, involving the gastrointestinal tract. We used the routine histological technique: samples fixed with 10% formalin, sections made with a microtome in 0.5mm section and then stained with haemateineosin. Finally, the slides are interpreted on a simple light microscope by an anatomopathologist. All TGI biopsies received during the study period are listed, assembled and analyzed. The results are presented in tabular form and graphs.
Results
Out of 221 histological samples received during the study period 100 concerned the digestive system (45.24%) (Figure I and II) and (Table I-VI).
The average age of the patients is 52.8 years (17-98 years). The most represented patients were those aged 60 and over (43.0%).
There is a slight predominance of women in our series, with an M: F sex ratio of 1: 1.3.
In our series, the most frequent localization of IGT disorders is gastric at 84%, and the rest distributed as follows: Esophagus (5%), Rectum (4%), Colon (4%), Duodenum (2%) and Pancreas (1%).
Out of 98 lesions recorded, 80.61% of lesions are inflammatory in nature against 19.39% of neoplastic lesions. Gastritis is the most common diagnosis (76.53%).
Inflammatory gastrointestinal pathology is distributed uniformly across all age groups, while malignant pathologies appear after 50 years.
Gastrointestinal malignancies are more frequent than men (20.93%) that women (3.63%) have a sex ratio of M: F of 3: 1.
The stomach is the most represented site, recording 84% of samples from the gastrointestinal tract, and recording 84.6% of all lesions in our study.
The lesions of the stomach are 89.29% gastritis; associated with atrophy (42.66%) and very often associated with Helicobacter pylori (94.66% of cases).
Discussion
The average age of our patients is 52.8 years (17-98 years). The most represented patients were those aged 60 and over (43.0%); see figure I. Our series is similar to the literature reported [9], in which the average age of patients was 55 years (23-80 years) with a higher frequency for the 40-60 year age group, unlike to that of some authors [10] whose mean age was 38.5 years (7-85 years), and 57% of patients with an age between 20 and 39 years. We note a slight predominance of women in our series, with an M: F sex ratio of 9:11 (Figure II), as in previous literature [11] whose M: F sex ratio was 107: 113, unlike another [10] which was predominantly male (sex ratio M: F of 707: 514).
Our study shows that the stomach is the most represented site, it stores 84% ??of samples from the digestive system see Table I. This trend is corroborated with the study by Nezha, which had a predominantly 40.74% gastric sample [9]. On the other hand, certain literature reports that digestive affections are very frequent in Africa with a strong predominance of colonic pathology [12,13].
80.61% of lesions in ourseries are inflammatory in nature see Table II. This percentage is very high compared to that found by Ndjitoyap et al, which was 54.65% [14]. This high frequency of inflammatory pathology in our context could be related to the multiple aggressive factors for the gastric mucosa which are part of the local diet of this population [15-18]. Indeed, of all the lesions observed in our study, gastritis is the most frequent diagnosis (76.53%). This frequency is higher than that reported with a predominance of gastritis at 27.79%. However, an ATTIA study in Ivory Coast reported twice as many duodenitis as gastritis [12].
An antecedent report finds malignant digestive diseases as the main cause of pathologies of this system with high mortality among all neoplasms, contributing to approximately 3 million deaths in 2012 worldwide. This report presents as the main digestive malignancies in descending order, hepatocellularcarcinoma (HCC), colorectal cancer, gastric cancer (GC), pancreatic cancer, cancer of the esophagus and oral cancer [18].
In our study we find a predominance of malignant lesions of the digestive tract in male patients with an M: F ratio of 3: 1 see Table IV. This opinion was reported by [19]. However, its incidence is characterized by a significant geographic disparity [20].
The inflammatory gastrointestinal pathology is distributed uniformly in all age groups while the malignant pathologies appear after 50 years see Table III. Malignant gastrointestinal lesions are more common in men (20.93%), with an M: F sex ratio of 3: 1 see Table IV. It seems clear to us that age is a risk factor for cancers of the gastrointestinal tract [16]. Indeed our result corroborates with some literature which reports that cancers of the gastrointestinal tract are rare before age 50 with a male predominance (sex ratio of 5: 2), and their incidence increases with age [16].
The stomach is the most affected site of TGI, it recorded 84.6% of all lesions in our study see Table V. This percentage is very high compared to that of [10], who had a predominance of gastric lesions at 44%.
In the lesions of the stomach are gastritis at 89.29% see Table VI and often associated with atrophy (42.66%) and very often associated with Helicobacter pylori (94.66% of cases), Helicobacter pylori being a major risk factor for gastric cancer according to several authors [21-23].
Conclusion
About 45.24% of the histological samples sent to the pathological anatomy department concern the digestive system. The inflammatory lesions of this system represent 80.61% of which 19.39% are neoplastic lesions. The cause of the predominance of inflammatory lesions remains to be determined. The most common diagnosis is gastritis, most often associated with Helicobacter pylori (94.66%). The eradication of Helicobacter pylori is very important in the strategy to combat digestive pathology.
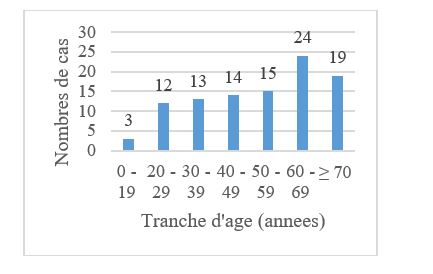
Figure I : Distribution of patients by age.
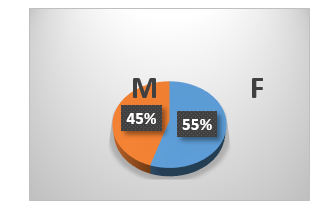
Figure II : Distribution of patients by sex.
|
Site |
Number of samples |
Percentage (%) |
|
Esophagus |
5 |
5.0 |
|
Stomach |
84 |
84.0 |
|
Duodenum |
2 |
2.0 |
|
Côlon |
4 |
4.0 |
|
Rectum |
4 |
4.0 |
|
Pancréas |
1 |
1.0 |
|
Total |
100 |
100.00% |
Table I : Distribution of samples by anatomical site.
|
Pathological diagnosis |
Workforce |
Percentage |
|
Adenocarcinoma |
8 |
8.0% |
|
Carcinoma |
2 |
2.0% |
|
Duodenitis |
1 |
1.0% |
|
Gastritis |
75 |
75.0% |
|
Lymphoma |
2 |
2.0% |
|
Esophagitis |
1 |
1.0% |
|
Benign polyp |
7 |
7.0% |
|
RCUH* |
2 |
2.00% |
|
Without lesion |
2 |
2.00% |
|
Total |
100 |
100.00% |
|
Note:*RCUH: ulcerative colitis. |
||
Table II: Distribution of samples according to pathological diagnosis.
|
Age range |
0 - 19 |
20 - 29 |
30 - 39 |
40 - 49 |
50 - 59 |
60 - 69 |
≥70 |
Total |
|
Pathological dg |
- |
- |
- |
- |
- |
- |
- |
- |
|
Adenocarcinoma |
- |
- |
- |
- |
3 |
5 |
- |
8 |
|
Carcinoma |
- |
- |
- |
- |
1 |
- |
1 |
2 |
|
Duodenitis |
- |
1 |
- |
- |
- |
- |
- |
1 |
|
Gastritis |
3 |
10 |
12 |
11 |
10 |
13 |
16 |
75 |
|
Lymphoma |
- |
- |
- |
- |
- |
2 |
- |
2 |
|
Esophagitis |
- |
- |
- |
- |
- |
- |
1 |
1 |
|
Benign polyp |
- |
- |
- |
1 |
1 |
4 |
1 |
7 |
|
RCUH |
- |
- |
- |
2 |
- |
- |
- |
2 |
|
Without lesion |
- |
1 |
1 |
- |
- |
- |
- |
2 |
|
Total |
3 |
12 |
13 |
14 |
15 |
24 |
19 |
100 |
Table III: Pathological diagnosis by age group.
|
Pathological diagnosis |
F |
M |
Total |
|
Adenocarcinoma |
1 |
7 |
8 |
|
Carcinoma |
1 |
1 |
2 |
|
Duodenitis |
- |
1 |
1 |
|
Gastritis |
48 |
27 |
75 |
|
Lymphoma |
1 |
1 |
2 |
|
Esophagitis |
1 |
- |
1 |
|
Benign polyp |
3 |
4 |
7 |
|
Proctocolitis |
- |
2 |
2 |
|
Without lesion |
- |
2 |
2 |
|
Total |
55 |
45 |
100 |
Table IV: Diagnostic pathology by Sex.
|
Site / Dg pathological |
Workforce |
Percentage |
|
Colon |
4 |
4.00% |
|
Adenocarcinoma |
1 |
1.00% |
|
Benign polyp |
1 |
1.00% |
|
RCUH |
1 |
1.00% |
|
Without lesion |
1 |
1.00% |
|
Duodenum |
2 |
2.00% |
|
Duodenitis |
1 |
1.00% |
|
Benign polyp |
1 |
1.00% |
|
Stomach |
84 |
84.00% |
|
Adenocarcinoma |
5 |
5.00% |
|
Gastritis |
75 |
75.00% |
|
Lymphoma |
2 |
2.00% |
|
Benign polyp |
1 |
1.00% |
|
Without lesion |
1 |
1,00% |
|
Esophagus |
5 |
5.00% |
|
Carcinoma |
2 |
2.00% |
|
Esophagitis |
1 |
1.00% |
|
Benign polyp |
2 |
2.00% |
|
Pancreas |
1 |
1.00% |
|
Adenocarcinoma |
1 |
1.00% |
|
Rectum |
4 |
4.00% |
|
Adenocarcinoma |
1 |
1,00% |
|
Benign polyp |
2 |
2.00% |
|
RCUH |
1 |
1.00% |
|
Total |
100 |
100.00% |
Table V: Pathological diagnosis according to anatomical sites.
|
Pathological diagnosis |
Workforce |
Percentage |
|
Adénocarcinome |
5 |
5.95% |
|
Gastritis |
75 |
89.29% |
|
Without atrophy |
43 |
51.19% |
|
Without H.p |
3 |
3.57% |
|
With H.p |
40 |
47.62% |
|
With atrophy |
32 |
38.10% |
|
Without H.p |
1 |
1.19% |
|
With H.p |
31 |
36.90% |
|
Lymphoma |
2 |
2.38% |
|
Benign polyp |
1 |
1.19% |
|
Without lesion |
1 |
1.19% |
|
Total |
84 |
100.00% |
Table VI : Stomach lesions.
Citation: Enow Orock G, Enow Orock A, Ngounou E, Konang N Jl, Noubom M, et al. (2020) Gastrointestinal Pathologies in a Center with Limited Resources: Pilot Study at Bafoussam Regional Hospital, Cameroon. J Surg Insights: JSI-100022
