
Emergency Medicine and Trauma Care Journal
ISSN 2652-4422
Case Report
Radial Nerve Entrapment caused by a Desmoid Tumor : A Case Report and Literature Review
Benabdallah O*, Benmoussa A, El Andaloussi Y, Haddad H and Benabdallah R
Avicenne University Hospital Center and Tangier Hospital Centers, Morocco
*Corresponding author: Otman Benabdallah, Avicenne University Hospital Center and Tangier Hospital Centers, Morocco.
Citation: Benabdallah O, Benmoussa A, El Andaloussi Y, Haddad H, Benabdallah R (2020) Radial Nerve Entrapment caused by a Desmoid Tumor : A Case Report and Literature Review. Emerg Med Trauma. EMTCJ-100049
Received date : 12 May, 2020; Accepted date : 30, May 2020; Published date : 05 June, 2020
Abstract
Case : We report a case of a 45 year's old woman with a radial nerve entrapment caused by a desmoid tumor involving the right forearm. This case is outstanding because of the posterior interosseous nerve is entrapped inside the tumor. The marginal excision of the mass while preserving the intratumoral radial nerve was laborious.
Conclusion :The radial nerve entrapment caused by a desmoid tumor is very rare and intratumoral radial nerve entrapment is also exceptional. The surgical treatment was challenging and the prognosis is uncertain because of the high rates of recurrence of the desmoid tumor.
Background: One case of radial nerve entrapment or posterior interosseous nerve palsy caused by a desmoid tumor is reported. This case is outstanding for two reasons:
Method: Clinical, radiological, histopathological data of the patient and relevant literature were reviewed.
Results: We report a case of a radial nerve entrapment caused by a desmoid tumor involving the forearm that was treated with operative excision.
Conclusion: Radial nerve entrapment caused by a desmoid tumor is very rare. As the desmoid tumor is a locally aggressive tumor the prognosis of the treatment is uncertain.
Keywords: Forearm desmoid utmor; Posterior interosseous nerve palsy; Nerve compression; Radial nerve entrapment
Introduction
Radial nerve entrapment can occur at any location within the course of the nerve distribution but the most frequent location of entrapment occurs in the proximal forearm. Radial nerve entrapment is secondary to different causes such as direct trauma, fractures, lacerations, compressive devices, tumors [1].
Local tumor compression is the main mechanical cause of posterior interosseous nerve palsy [2-4]. Here we report a case of a 45 year's old woman with more than one-year history of painful swelling, paresthesia and progressive weakness of her right hand. Plain radiography, CT and MRI identified a tumor; the electromyography revealed the nerve palsy with denervation and histological examination confirmed the diagnosis of desmoid tumor. We performed a complete resection of the mass which was intertwined in surrounding tissue with the nerve entrapped inside the tumor making the resection very challenging. This condition of intratumoral radial nerve entrapment is exceptional.
Following removal of the mass the patient recovered complete function of her right hand.
Among compressive tumors of radial nerve, the desmoid tumor should be considered as an exceptional cause of radial nerve palsy. To our knowledge no previous radial nerve entrapment caused by a desmoid tumor has been reported in the literature [4-7].
The patient was informed that data concerning the case would be submitted for publication, and she provided consent.
Case report
A 45 year’s old woman presented with painful swelling of the forearm with gradual increase in size,paresthesia and progressive weakness of her right hand. There was no history of trauma or infection. Physical examination revealed a firm, non- tender mass at the upper third of the forearm. Range of motion of the elbow and the wrist were preserved; she had some difficulties to extend their fingers. Sensory disturbance was observed on the postero-external side of the forearm.
Plain radiography showed a tissue mass.Magnetic resonance images [8] revealed a mass involving the posterior and lateral muscular compartment of the forearm measuring 7.57 cm in vertical axis and 6.7 cm in tranversal axis. This mass consists of irregular shape and lobulated contours.T1 weighted images revealed low signal intensity and T2 weighted images revealed a high signal intensity with a strong enhancement after administration of Gadolinium. On the other hand, the posterior interosseous nerve and the radius were surrounded by this mass (Figure 1).
Microscopic examination of the removed tumour revealed that the tissue is composed of spindle shaped cells made by fibroblasts and myofibroblasts separated by abondant collagen tissue.The cells don't show cellular atypia and have a weak mitotic index (Figure 2). The tumor contour is surrounded by an atrophic muscular tissue.
Marginal excision of the mass was performed through an anterior approach with external curved incision (Figure 3).
The mass was intertwined in surrounding tissue, muscles, radial bone and the most important surrounding the posterior interosseous nerve (PIN) which nerve was imprisoned inside the tumor(Figure 4) making the decompression of the nerve and the excision of the tumor very laborious and very challenging. In practice we splitted the tumor in two parts and then partitioned the tumor in multiple parts to liberate the imprisoned radial nerve. We followed the path of the nerve with an electrical stimulator used by the anesthesiologists for regional anaesthesia. The mass was removed and the nerve liberated successfully.
We do not perform any complementary therapy. The patient ‘s radial nerve palsy improved after the removal of this tumor and has a restoration of normal function of her right hand;but she keeps some sensory troubles on the back of the arm during four months.
Regarding follow up, the patient was first seen 13 months ago and has been operated on and followed for 12 months.
Discussion
This case is outstanding for two reasons: there is no prior study reporting a desmoid tumor as a cause of radial nerve entrapment and no prior study reporting an intratumoral entrapment.
The PIN may be affected by various lesions in the forearm:radial tunnel, tumors,trauma, miscellaneous lesions,rheumatoid arthritis. Quignon[5] and Kohyama[2] reported tumor compression as the main etiology of PIN palsy with a rate of 39,4%.
In our case concerning the diagnosis of a desmoid tumor, to our knowledge no one has reported a PIN palsy caused by a desmoid tumor. This tumor was identified by radiological exams (X-ray, CT and MRI) and certitude diagnosis was confirmed by histological examination after marginal excision. Desmoid tumors also called aggressive fibromatosis are benign tumors,but locally aggressive and with a high rate of recurrence[9,10]. They are very rare tumors;among extra-abdominal desmoid tumors, the location in the forearm is about 4%; they do not metastasize to other parts of the body, however one case of pulmonary metastasis secondary to a location in the foot was reported[11]. But these tumors can locally grow aggressively and become intertwined in surrounding tissue as our case in which radial nerve was imprisoned inside the tumor, radial bone surrounded and muscles intertwined making it very difficult to remove surgically. And even apparently complete surgical removal desmoid tumors frequently grow back. So the prognosis of our case is uncertain.
The PIN is a motor nerve,however it gives off terminal sensory branches to the ligaments and articulations of the carpal joints,to the periosteum of the radius and interosseous membrane of the forearm explaining the aching pain and sensory disturbance in our patient. In addition, as the superficial radial nerve passes above the supinator muscle it was also compressed by the mass causing paresthesia along the way of the nerve to the anatomical gutter.
Treatment of extra abdominal desmoid tumors consists of radiation therapy, chemotherapy,cryotherapy, antiestrogens,surgical excision [12-16].In our case treatment involved complete resection because of the compression of the PIN and patient’s suffering. Management of these lesions is complex,the main problem being the high rates of recurrence.Surgical decompression was recommended in our patient and a rapid recovery was obtained but the prognosis is uncertain. So a regular overnight must be maintained.
Conclusion
This case is outstanding for many reasons
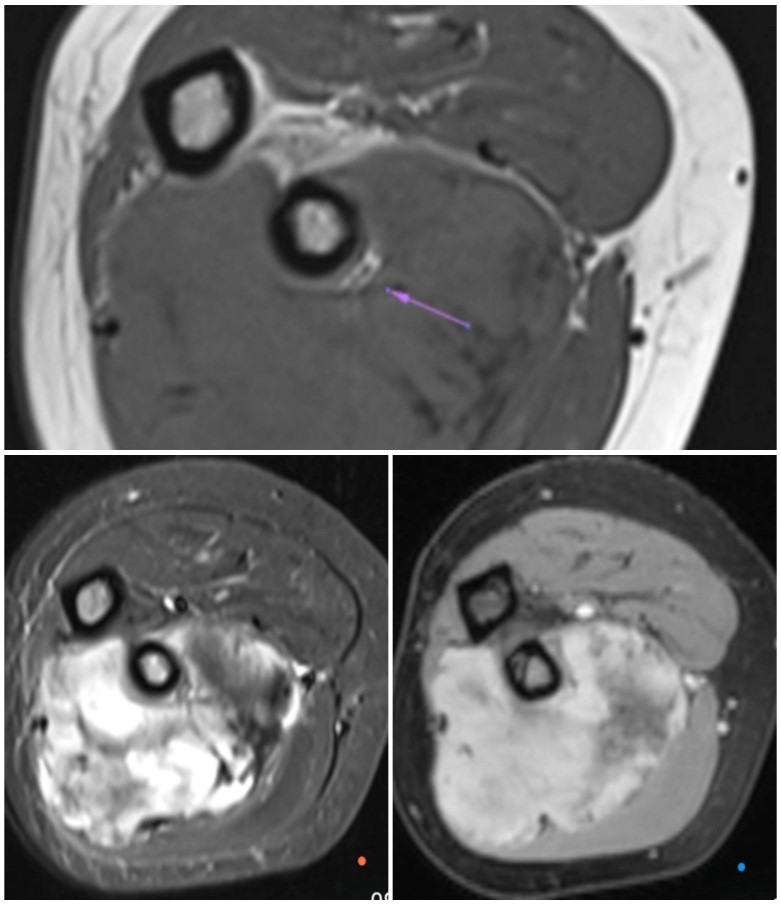
Figure 1: T1 weighted image,T2 weighted image with fat saturation and T1 weighted image with fat saturation after Gadolinium administration.The image above shows the radial nerve entraped inside the tumor.
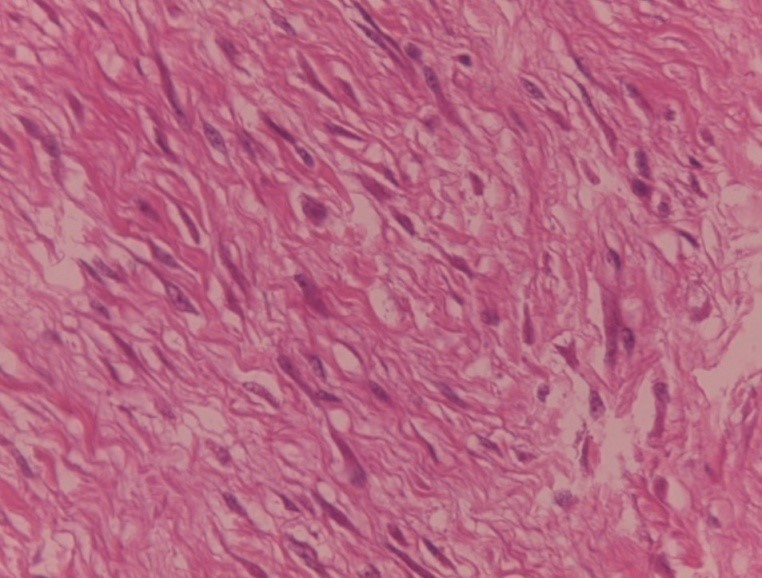
Figure 2: Microscopic examination revealed that the tissue is composed of spindle shaped cells made by fibroblasts and myofibroblasts separated by abondant collagen tissue.
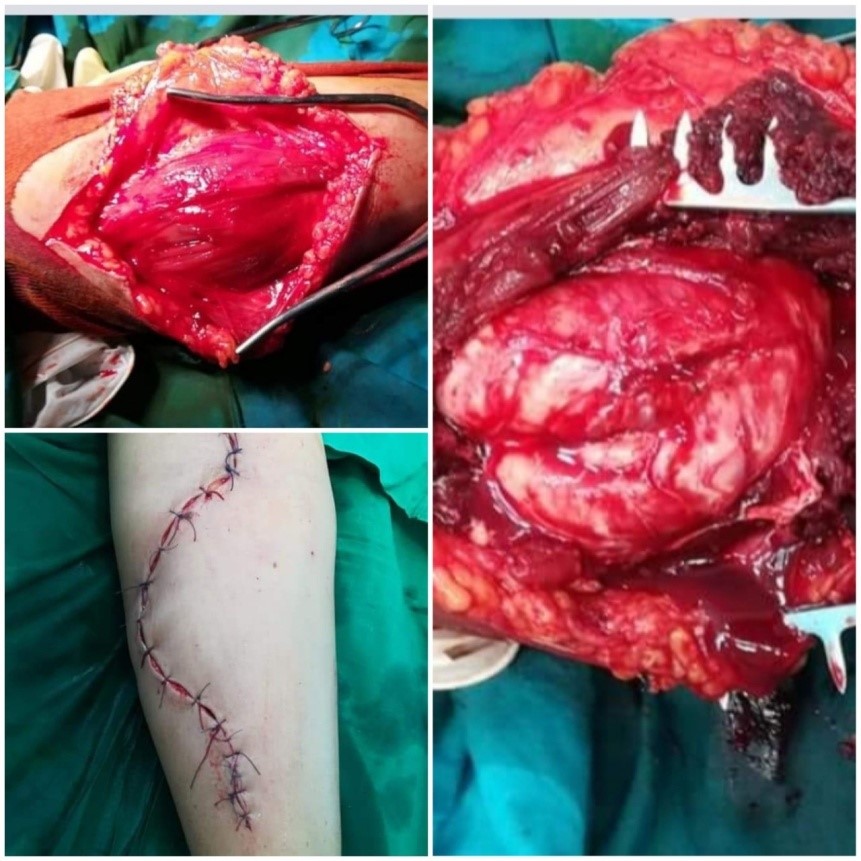
Figure 3 :Marginal excision by anterior approach using a curved incision.
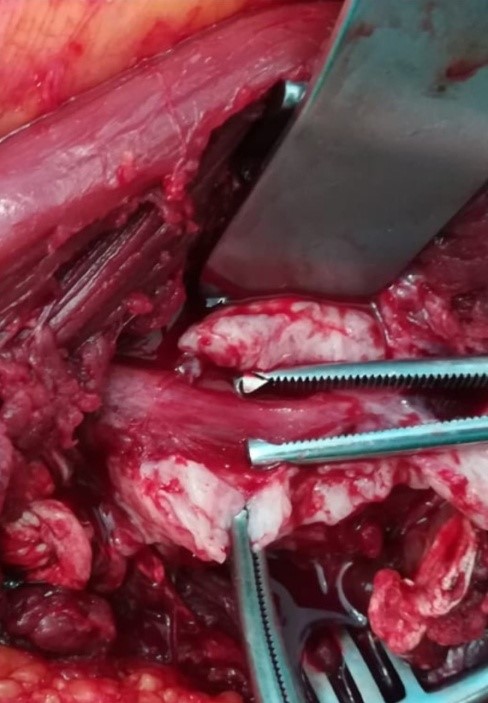
Figure 4 :Intra-operative image showing the radial nerve entraped inside the tumor.
Citation: Benabdallah O, Benmoussa A, El Andaloussi Y, Haddad H, Benabdallah R (2020) Radial Nerve Entrapment caused by a Desmoid Tumor : A Case Report and Literature Review. Emerg Med Trauma. EMTCJ-100049
