
Journal of Surgery and Insights
(ISSN 2652-4643)
Clinical Image
Neuroendocrine Mammary Carcinoma
Abdel Hadi M*, Al Muhanna A and Ahmed A
Departments of Surgery, Radiology and pathology, Imam Abdulrahman Bin Faisal University Dammam, Saudi Arabia
*Corresponding author: Maha Abdel Hadi, Department of Surgery, Imam Abdulrahman Bin Faisal University Dammam, Saudi Arabia.
Citation: Abdel Hadi M, Al Muhanna A, Ahmed A (2020) Neuroendocrine Breast Carcinoma. J Surg Insights: JSI-100019
Received date: 22 April, 2020; Accepted date: 25 April, 2020; Published date: 30 April, 2020
Introduction
Mammary neuroendocrine tumors are an under recognized entity. High occurrence is noted in postmenopausal women. For ease of description, they may be classified into well differentiated, poorly differentiated neuroendocrine tumors, or invasive breast carcinoma with neuroendocrine features. [1] The diagnosis remains a challenge. The key is to employ the available biomarkers and radiological imaging to confirm the diagnosis. Immunohistochemistry aids to document the expression of the neuroendocrine markers synaptophysin [2]. The high sensitivity, specificity and the accuracy of Tc-99m-OCT scan essential for the diagnosis and follow-up [3]. With the aid of both immunohistochemistry the Tc-99-OCT the diagnosis of this clinical case was reached.
Clinical Case
A young lactating mother presented with an expanding breast mass of few months’ duration. Physical examination and Standard workup were unremarkable. Breast imaging demonstrated a well circumscribed mass. Core biopsy showed an undifferentiated malignant neoplasm with hyperchromatic, pleomorphic cells, abundant mitosis, increased vascularity and areas of necrosis (Figure I).
Technetium-99m -Octreotide scan demonstrated an uptake in the large left breast mass and the largest left axillary node. Both sites were consistent with positive somatostatin receptor (SSR) lesions (Figure II a,b).
Distal metastatic workup was negative. Immunohistochemically analysis, reported S100, CD-56 and synaptophysin as positive (Figure III).
Based on the morphological features, the immune cytochemical markers and Octreotide avid uptake the diagnosis of Poorly differentiated Invasive Neuroendocrine Carcinoma was confirmed.
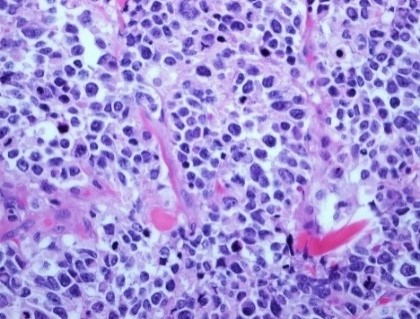
Figure I: 40X Microscopic picture showing tumor with prominent vascularity and focal rosette formation, many mitosis and cell apoptosis.
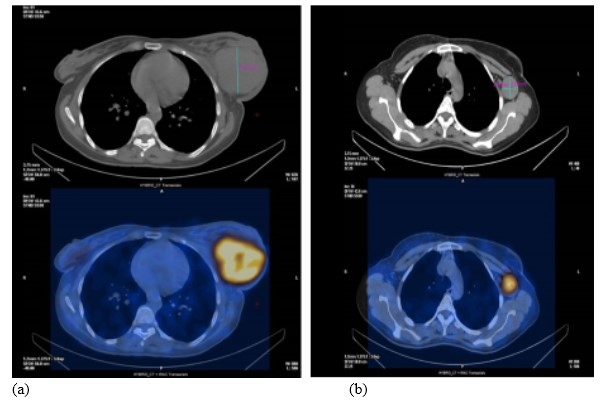
Figure II a,b: SPECT-CT Axial fused and CT slices of the chest and axillae. Demonstrates heterogeneous increased uptake in the large left breast mass and largest left axillary node.
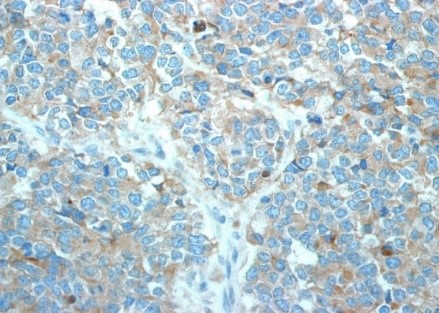
Figure III: 20X showing tumor cells positive for synaptophysin.
Citation: Abdel Hadi M, Al Muhanna A, Ahmed A (2020) Neuroendocrine Breast Carcinoma. J Surg Insights: JSI-100019
