
Journal of Surgery and Insights
(ISSN 2652-4643)
Case Report
Surgical Stabilisation of Unstable Thoracic Spine and Rib Fractures with a Single Anaesthetic in a Multi-Trauma Patient
Fagg D1*, Hampson-Tindale G1, Jonathan A2, Wullschleger M1 and Patel B1
1Division of Trauma Surgery, The Gold Coast University Hospital , Gold Coast, Queensland, Australia
2Division of Neurosurgery, The Gold Coast University Hospital, Gold Coast, Queensland, Australia
*Corresponding author: Damen Fagg, Division of Surgery, Gold Coast University Hospital, Queensland, Australia.
Citation: Fagg D, Hampson-Tindale G, Jonathan A, Wullschleger M and Patel B (2020) Surgical Stabilisation of Unstable Thoracic Spine and Rib Fractures with a Single Anaesthetic in a Multi-Trauma Patient. J Surg Insights: JSI-100017
Received date: 20 March, 2020; Accepted date: 23 March 2020; Published date: 30 March, 2020
Introduction
A 73-year-old male was brought to the Emergency Department of our Level I trauma centre following a fall from eight metres. On arrival, the patient had a respiratory rate of 32 breathes per minute with oxygen saturations of 97% on 15L of oxygen via a non-re-breather. There was no neurological deficit in the upper or lower extremities. Computed Tomography (CT) trauma series revealed multiple displaced bi-cortical right and minimally displaced left sided rib fractures with associated small pnuemothoracies and multiple thoracic vertebral fractures from T6-T12 (Figure1,2).
The T12 vertebra associated burst fracture had approximately 30% loss of height anteriorly and approximately 40% loss of height centrally. The fracture extended posteriorly into the left lamina, pars interarticularis and just into the superior articular facet. There was also 3 mm of retropulsion which resulted in minor canal stenosis. The CT brain demonstrated a subdural hematoma with no midline shift. A type II respiratory failure and worsening metabolic acidosis over the next 48 hours led to intubation and ventilatory support in the Intensive Care Unit (ICU).
Following a multidisciplinary discussion between trauma surgery, thoracic surgery, neurosurgery and the intensive care physicians, the patient underwent a combined procedure with a general anaesthesia using a single lumen tube for reduction and fixation in the prone position. The patient had a pedicle screw fixation of T8-L2 followed by open reduction and internal fixation of the right ribs 3,4,5,6,7 and 9 (Figure 3) via a second incision parallel to the medial border of the scapula. There were no associated intraoperative or post-operative complications. The patient was discharged from the intensive care unit on day 50 for ongoing rehabilitation and furthermore, discharged home from hospital on day 70 of admission.
Discussion
We hereby report a case of unstable thoracic spine and rib fractures successfully managed in prone position as a combined case via a single lumen general anaesthetic. Rib fractures are very common in trauma and, in addition to being associated with other thoracic injuries, they are often associated with concomitant abdominal, head and extremity injuries [1]. They are associated with significant morbidity and mortality, with mortality rates as high as 33%2.
There are several advantages of early fixation including lower rates of pulmonary complications and thromboembolic events, reduced intensive care stay with fewer ventilated days and reduced opioid requirements [2].
Indications for rib fixation include a flail chest requiring mechanical ventilation, however many centres use a broader criterion that address patients who do not have a flail chest but rather those who have respiratory compromise, rib fracture non-union or during a thoracotomy performed primarily for other reasons [3].
Rib fractures are commonly repaired in the lateral decubitus position, however, depending on the fracture location and other traumatic injuries, fixation can be either done in the prone or supine position. A literature search revealed limited data with regards to combined cases of rib fixation and thoracic spine stabilisation.
In our case, fixation and stabilisation was achievable due to cautious multidisciplinary approach between neurosurgery, trauma surgery, thoracic surgery, ICU team and the anaesthetic team to ensure a successful outcome via a single visit to the operating theatre.
With careful patient section and planning, both unstable thoracic and rib fractures can be managed with a single anaesthetic. A cautious multidisciplinary team approach is necessary to ensure a satisfactory outcome and coordination of management. This approach not only eliminates the need for a second anaesthetic and utilisation of further resources but aims to reduce the patient’s morbidity and mortality. As a result of early fixation, the patient may benefit from reduced time in intensive care, decreased opioid requirements and a reduction in the morbidity and mortality associated with respiratory and thromboembolic complications.
Disclosure Statement: I her by declare that there are no financial or any other conflicts of interest associated with this publication.
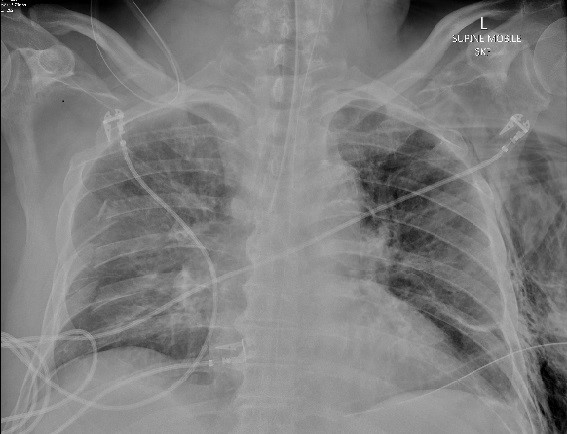
Figure 1: Supine chest x-ray study demonstrating right lateral and posterior rib fractures.
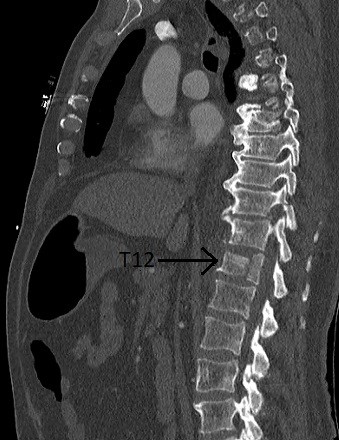
Figure 2: Sagittal thoracic CT image demonstrating an unstable three column thoracic fracture at the level of the 12th thoracic vertebra.
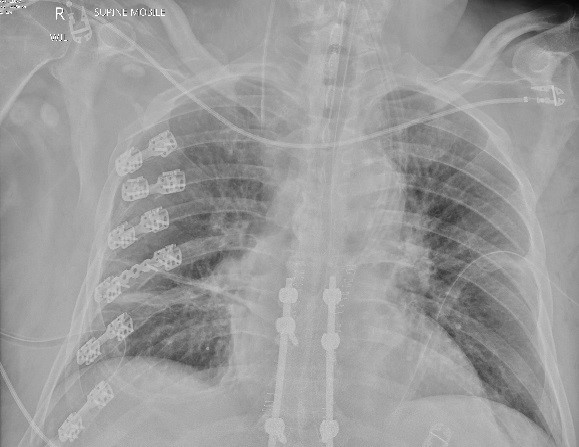
Figure 3: Supine chest x-ray study demonstrating fixation of right posterior lateral rib fractures and the thoracolumbar spine.
Citation: Fagg D, Hampson-Tindale G, Jonathan A, Wullschleger M and Patel B (2020) Surgical Stabilisation of Unstable Thoracic Spine and Rib Fractures with a Single Anaesthetic in a Multi-Trauma Patient. J Surg Insights: JSI-100017
