
Journal of Surgery and Insights
ISSN 2652-4643
Case Report
Surgical Reconstruction of the Nose in Sub Saharian Country: A Propos of 27 Cases
Ndiaye Lamine1*, Ndiaye Aïnina1, Touré Silly2, FobaMamadou Lassana1 and Sankalé Anne-Aurore1
1Department of Plastic Surgery, Aristide Le Dantec Hospital, Senegal
2Department of Maxillo-Facial Surgery, Aristide Le Dantec Hospital, Senegal
*Corresponding author:LamineNdiaye,Department of Plastic Surgery, Aristide Le Dantec Hospital, Senegal, Tel: +221 777164949; Email: drlndiaye@yahoo.fr
Citation: Ndiaye L, Ndiaye A, Toure S, Foba ML, Sankale AA (2020) Surgical Reconstruction of the Nose in Sub Saharian Country: A Propos of 27 Cases. J Surg Insights: JSI-100010 Received date: 07 February, 2020; Accepted date:14 February, 2020; Published date: 21 February, 2020
Abstract
Background: Nose reconstruction is a very challenging procedure in our context and the are still rising in our department. Nose defect lead aesthetical concern.Patients are mostly young women victims of injuries. The aim of this study was to report our experience reconstruction of nose defect.
Patients and Methods:We carry out a retrospective study from January 2002 to December 2019. Thirty to patient with nose following different aetiologias were included. Patients with cleft lip were exclude. Parameters studied were epidemiologic, clinic and therapeutic.
Results:There was 13 men and 14 females. Mean age was 27yrs [7month -57 yrs].Aetiologias was dominated by human bite in 7 cases, noma sequela 6 cases, burn in 4 cases, road traffic injuries 4 cases, benign tumor 3 cases and malign tumor 3 cases.
The loos of substance involved the alar in 15 cases, the columella in 4 cases, both alar and columella in two cases, the dorsum in 4 cases and the alar and dorsum in 2 cases.Fourteen patients have been operated of which 6 alar reconstructions by nasolabial flap and composite auricular helix graft, 2 columella reconstructions by local flap, 2 cases of nasal remodeling after neurofibroma removal, 2 dorsum reconstruction by local flap, one forehead flap for columella and alar reconstruction and one full thickness skin graft.
Complications occurred in 4 cases. We had one case of composite graft loss, partial forehead flap necrosis and 2 hypertrophic scars. After 5 months’ mean follow up, results were assessed as excellent in 4 cases, good in 7 cases and fair in 3 cases.
Conclusion: Reconstruction of the is challenging in young women people who may have disgraces scars such us keloids or hypertrophic scar. The chosen procedure should be simple and lead to the lowest sequela.
Keywords: Nose defect; Reconstruction; Sub-Saharan people; Surgery
Introduction
The nose is the most prominent organ of the face and every little anomalymay cause an importantconcern.The aetiologia of nasal defect depend to population area. Reconstruction of nasal defect represent a difficult challenge in consideration of his situation, anatomy and function. In Caucasian people cancer removal is the main whereas in our daily practice, injuries are most seen. The purpose of reconstructing a loss of substance from theface, in this case the nose, is to allow the restoration as natural as possible by replacing each fabric with its best equivalent [1].
There are numerous procedures of nose reconstruction and the best technique should take account to the aesthetic unit as described by Burget[2]. Nose reconstruction is very challenging in our context because it is not often. Through this study we, we report our experience in nose reconstruction in sub-Saharan country.
Patients and Methods
We carry out a retrospective study from January 2002 to December 2019. During this period27 patients who needed nose reconstruction were included. Patients who undergone cleft lip and patient who did not need reconstruction were excluded.Data recording was made with medical files as well as pre and post-operative photographies.All procedures were performed under general anesthesia.
Results
There was 13 men and 14 females. Mean age was 27 [7month -57 yrs].Aetiologias was dominated by human bite in 7 cases, noma sequela 6 cases, burn in 4 cases, road traffic injuries 4 cases, benign tumor 3 cases and malign tumor 3 cases.The loos of substance involved the alar in 15 cases, the columella in 4 cases, both alar and columella in two cases, the dorsum in 4 cases and the alar and dorsum in 2 cases.
Fourteen patients have been operated of which 6 alar reconstructions by nasolabial flap and composite auricular helix graft, 2 columella reconstructions by local flap, 2 cases of nasal remodeling after neurofibroma removal, 2 dorsum reconstruction by local flap, one forehead flap for columella and alar reconstruction and one full thickness skin graft.
Complications occurred in 4 cases. We had one case of composite graft loss, partial forehead flap necrosis and 2 hypertrophic scars. After 5 months’ mean follow up, results were assessed as excellent in 4 cases, good in 7 cases and fair in 3 cases.
Discussion
Nasal loss of substance requires aesthetic and functional reconstruction to allow better social well-being. The chosen technique should let the lowest sequela to avoid post-operative concerns. The aetiologies of the nasal defect are numerous and depend to the geographic area. In our study, injuries such as human bite, road traffic injuries and burns were most seen. However, in western countries tumor removal are more often[3]. As same as in our study, [4] recommends to perform all procedures under general anesthesia because it permits the intraoperative evaluation of vascularity and three-dimensionalcontour without vasoconstriction or fluid distortion.Nose reconstruction is based on three principles: make a precise diagnosis of the loss of substance, replace each tissue with its best equivalent, respect the aesthetic units [1].
In our study, the transfixing loss of substance involved mainly the alar wing and the columella. Reconstruction of these units are one of the most difficult procedures in facial plastic surgery [5].For the alar reconstruction we did use two kind of procedures: the superiorly based nasolabial flap, describe by Burget and composite graft from the auricular helix root. The superiorly based naso-labial flap is a safe and good technique for the reconstruction of transfixing loss of substance and allows to obtain an excellent postoperative result, both on the aesthetically and functionally[6]. However, there are some inconvenient such as extra scar, and additional procedures for flap weaning or for degreasing the flap[7].
The composite auricular helix graft can also be use in defect less than a centimeter. In the literature [8-10], losses of nasal substance less than 1 cm wide, the composite chondro-cutaneous graft, taken at the root of the auricular helix constitutes the reference technique described. The composite graft failure we noted was probably due to an insufficiency of scar tissue excision.Care should be therefore taken to excise the cicatricial tissue of the bank of the defect to allow graft take. There is no additional scar on the nose and the face. The end result is then higher than that obtained by the best reconstructions by flap, due to the finesse, the precision of the nasal contour andof the lighting of the delicate modeling of the two "domes" under an ideal skin [1]. For the one case of columella reconstruction, we did perform a local flap introduced by Elbaz[11].It’s a simple procedure which is suitable for people with large nostril as we can see it in black people. The forehead flap we did realize was due to the fact that previous failed reconstruction had compromised the use of local flap and the nose defect was both on the alar and the columella. Coloration, texture, thickness, suppleness makes frontal integumentsa privileged donor area for nasal reconstruction, as soon as extent of substance loss exceeds possibilities of flaps local. Proximity to the forehead and the quality of its axial vascular supply vertical allow the paramedian frontal flap to be used in all situations, from reconstruction of the nose wing to total nasal reconstruction [1].
Numerous techniques are available for nasal reconstruction. Reconstruction in cicatricial tissue are very difficult due to contracture of surrounding tissue. The best result we obtained was in immediate reconstruction in tumor removal(Figure 1-5).
Conclusion
Nose reconstruction in sub Saharan and developing country is very challenging. Aetiologia are mostly due to injuries and young people are mainly affected. The chosen technique should provide best social well-being and the lowest morbidity.
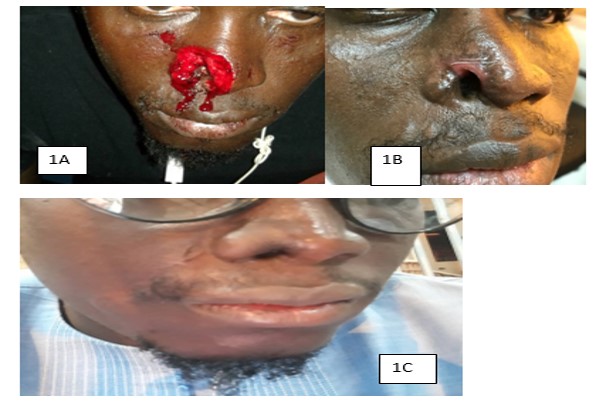
Figure 1: Reconstruction of alar defect following bite.
Figure 1A: Acute wound after bite.
Figure 1B: Alar defect after healing.
Figure 1C: 6 months follow after reconstruction by naso-labial flap described by BURGET.

Figure 2: Burn alar contracture.
Figure 2A and 2B: Alar post burn contracture.
Figure 2C: Alar reconstruction by composite auricular helix graft.

Figure 3: Dermoïd cyst of the dorsum.
Figure 3A: benign tumor of the dorsum.
Figure 3B: Immediate result after reconstruction by Rieger flap.
Figure 3C: Result after 3 years follow up.
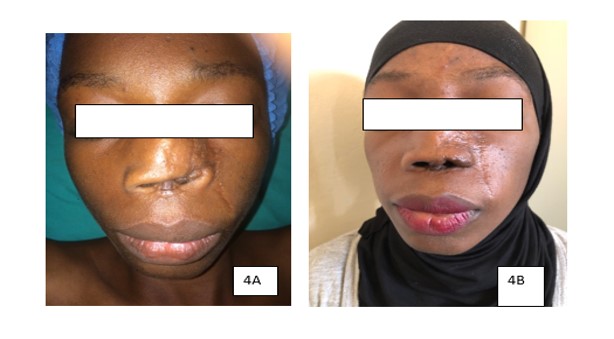
Figure 4: Alar and columela defect reconstrued by forehead flap.
Figure 4A: Alar and columela defect.
Figure 4B: 1yr follow up after forehead flap.

Figure 5: Plexiform neurofibroma of the nose.
Figure 5A:Neurofibroma of the alar and the dorsum.
Figure 5B: Immediate result tumor removal and nose remodeling.
Citation: Ndiaye L, Ndiaye A, Toure S, Foba ML, Sankale AA (2020) Surgical Reconstruction of the Nose in Sub Saharian Country: A Propos of 27 Cases. J Surg Insights: JSI-100010
