
Annals of Medical & Surgical Case Reports
(ISSN: 2652-4414)
Myocardial Bridges a Review of the Imaging Studies for Diagnosis
Ibarrola M*
Centro Cardiovascular BV, Piñero 883, Bella Vista, 1661, Buenos Aires, Argentina
*Corresponding author: Martin Ibarrola, Centro Cardiovascular BV, Piñero 883, Bella Vista, 1661, Buenos Aires, Argentina.
Citation: Ibarrola M (2020) Myocardial Bridges a Review of the Imaging Studies for Diagnosis. Ann Med & Surg Case Rep: AMSCR-1000033
Received date: 23 December, 2019; Accepted date: 10 January, 2020; Published date: 29 January, 2020
Abstract
Myocardial bridging (MB) is a congenital coronary anomaly in which a segment of a coronary artery takes a “tunneled” intramuscular course under a “bridge” of overlying myocardium. The first reference of MB in coronary arteries and the association with angina was referred by Reyman in 1737. Considered a benign finding since the myocardial bridge causes coronary artery narrowing during systole therefore myocardial bridges should not compromise blood supply to the musculature during diastole. The left anterior descending coronary (LAD) is the most frequently affected vessel (70% in an autopsy series) and in some cases hearts contain more than one bridge, affecting the same vessel or different coronaries.
Myocardial bridge is a clinical condition with several possible manifestations. It has been related to angina, myocardial infarction, arrhythmia, depressed left ventricular function, left bundle branch block, myocardial stunning, apical ballooning syndrome, early death after cardiac transplantation, and sudden death.
The classification proposal by Schwarz based on Clinical-Angiographic Data and Long- Term Follow-Up in angiographic findings and relationship with symptoms only in MB over the LAD, if used for decision making. Another technology such as intravascular ultrasound and valuation in Fractional flow reserve or Cardiac computed tomography angiography (CCTA) they allow to visualize the coronary anatomy of MB not only in LAD besides that study in another artery (branch arteries) and another congenital coronary anomaly. The clinical applications of these imaging methods a used for the diagnosis in congenital coronary anomalies is a review.
Keywords: Coronary angiography; Cardiac computed tomography angiography; Myocardial ischemia; Myocardial bridging
Introduction
The first reference of MB was Reymann, H, the anatomically description Published in the Dissertational inauguralem De Vasis Cordis Propriis, written in Latin, described anatomically the presence of MB in a description and their relationship with angina in 1937. When noted this anatomy in human heart. Described was a congenital variant of a coronary artery in which a portion of an epicardial coronary artery (most frequently the middle segment of the LAD takes an intramuscular course [1]. The relation of MB in coronary arteries and presence of angina was described in 1796 [2]. An in-depth analysis of autopsy samples was presented by [3]. In 1960 Porstmann W publish “The mural coronary” described abnormal finding of MB in the angiographic study [4]. In 1961, Polacek was the first to use the term “myocardial bridge” when described these formations calling them as MB, referred occur in 85.7% of all hearts; the occurrence is more frequent in the region of the left coronary artery in a study of 70 patients [5]. Different anatomical variants are presented in the called MB.
Described the clinical significance of isolated coronary MB such has benign and frequent condition involving the left anterior descending artery in asymptomatic patients without angina and presence of MB in angiographic study [6].
In a study of coronary angiograms of 64 hearts transplant patients were reviewed to determine the incidence of myocardial bridges. Only in 33% of these patients, myocardial bridges were detected, almost exclusively across the mild portion of the left anterior descending coronary artery. This is an evidence for the poor angiography for the diagnostic of MB except in the LAD [7].
The MB also has been associated with angina, [8] myocardial infarction, [9] arrhythmia [10], depressed left ventricular function, left bundle branch block [11], myocardial stunning, [12], apical ballooning syndrome, (13) early death after cardiac transplantation, and sudden death [14].
In a meta-analysis in MB were included 2519 articles and analyzed 21 articles of these. The presence of MB led to a significantly increased risk for Major Adverse Coronary Events (MACE) and myocardial ischemia [15].
Morphology
Represent an anomaly of coronary artery flow in which the branches flowing subepicardial descend into the myocardium shallower or deeper, and after a shorter or longer intramyocardial flow, it reappears in the subepicardial tissue (Figure 1).
Bundles of myocardial fibers, which in the form of small bridges, pass over the corresponding part of the coronary artery (“tunnel” segment), are marked as the MB [16].
Myocardial bridges are most commonly localized in the middle segment of the LAD, in another reports the anatomical variant of ramus intermedius artery presents MB [6,11]. Diagonal and marginal branches may be involved in 18% and 40% of cases [17]. Also has reported used the presence of multiple myocardial bridges and left ventricular dysfunction with Cardiac computed tomography angiography associated with left bundle branch block, in a patient with angina and positive stress test [11] (Figure 2).
They are distinguished between two types of bridging: superficial bridges (75% of cases) crossing the artery perpendicularly or at an acute angle toward the apex, and muscle bundles arising from the right ventricular apical trabeculae (25% of cases) that cross the LAD transversely, obliquely, or helically before terminating in the interventricular septum (Figure 3).
Pathophysiology and relationship with atherosclerosis
Only 15% of coronary blood flow occurs during systole paradoxically MB is a systolic finding for diagnostic in angiography study. Obviously, this allows only recognizing the muscle bridges in the main coronary arteries. In coronary angiograms are to be detected indirectly, based on the systolic reduction of lumen. The tachycardia may worsen ischemia because of a decrease in diastolic filling time and in coronary flow reserve [19]. MB have been described as super?cial or deep on the basis of: a) they range from 0.3 to 28mm in depth, b) anatomically they consist of either super?cial myocardial ?bers that traverse over the LAD or deep ?bers that encircle the LAD (5,7), and c) bridges >5 mm deep are less amenable to surgical myotomy. The hemodynamic impact of myocardial bridging depends on the thickness and length of the bridge, the orientation of the bridge relative to myocardial ?bers, and the presence of loose connective or adipose tissue around the bridged segment [18,20].
Coronary artery spasm is not an uncommon and has been recognized as an important cause of chest pain in patients with normal or non-significant obstructive coronary artery disease and the association of this with MB was also reported [21]. Physiologic evaluation of myocardial bridging performed with dobutamine and evaluated the Fractional flow reserve, evidenced such as dobutamine increased the morphologic and functional severity of MB [22].
This is evidential by Schwarz E performed a study in patients with chest pain, angiographic MB of the left anterior descending artery without obstructive coronary artery disease. Patients were evaluated for clinical symptoms, objective signs of ischemia by stress test, intracoronary Doppler flow measurement and coronary flow reserve. Coronary flow reserve was significantly higher proximally compared with segments distal to the MB. The classification for symptomatic patients with MB: Type A: incidental finding on angiography, no objective signs of ischemia; Type B: objective signs of ischemia, and Type C: with or without objective signs of ischemia and altered intracoronary hemodynamics (by QCA/CFR/intracoronary Doppler). Types B and C responded well to β-blockers or calcium channel antagonists. Patients with type C refractory to medical therapy were treated with stenting of the MB [23].
Imaging Techniques for diagnostic and study of MB
The historic gold standard for diagnosing myocardial bridges is coronary angiography (CA) with the typical milking effect and a step down–step up phenomenon induced by systolic compression of the tunneled segment (Figure 4).
In coronary angiograms MB are to be detected indirectly, based on the systolic reduction of lumen and the milking effect may be missed. The limited frequency of myocardial bridging observed angiographically (0.5% to 16%) is in contrast with that of autopsy studies, which have reported a frequency of 40– 80%. Used intracoronary ultrasonography (IVUS) allows an accurate assessment of vascular anatomy. With Doppler studies, the coronary flow reserve measured proximal to the myocardial bridge was normal or slightly reduced and that distal to the bridge was impaired. With the low rate of diagnosis referred by angiography the IVUS; it’s an excellent method for studying MB, but not performed for routine diagnosis of these [24] (Figure 4).
MB can also be visualized with the use of novel noninvasive imaging techniques such as electron beam tomography (EBT) and Cardiac computed tomography angiography (CCTA) (Figure 5, 6).
The CCTA has as a non-invasive alternative for evaluation of coronary anatomy with a lower referral threshold than coronary angiography. In a study with the analysis in morphological features of coronary anomalies can be evaluated more precisely by CCTA than by CA, which might lead to a higher identification of congenital coronary anomalies in CCTA compared to CA. The prevalence of coronary anomalies was 7.9% in CCTA group and 2.1% in CA. The most commonly coronary anomaly detected by CCTA was myocardial bridging 42.8% and with CA 21.2%.
The authors concluded that the prevalence of coronary anomalies is substantially higher with CCTA than CA even after exclusion of patients with myocardial bridging which is more frequently found with CCTA. The CCTA is considered the primary imaging modality to detect and characterize the anatomy of coronary artery anomalies (CAA). It has a higher rate of detection of CAA than invasive coronary angiography and other noninvasive imaging modalities, because three- dimensional visualization of the entire coronary tree allows accurate depiction of the origin, course and ending of the coronary vessels [25]. Whenever knowledge of the anatomy of the cardiac vessels is crucial, CCTA represents a highly valuable noninvasive modality because of its capability to visualize the coronary arteries accurately and three- dimensionally, yielding a higher detection rate over invasive coronary angiography (Figure 7, 8). Because of its noninvasive nature, relatively low cost and low radiation exposure, a further increase of the utilization of CCTA may be expected, which may consequently be paralleled by an increasing absolute number of incidentally detected CAA [15,26].
Diagnosis and Therapeutic approaches
Medical treatment of MB includes β-blockers with decrease the tachycardia and increase diastolic time, with a decrease in contractility and compression of the coronary arteries.
Calcium channel blockers and stents [27]. The frequency of in-stent restenosis requiring target vessel revascularization was 36% and high inflation pressures may be required for optimal stent implantation, with a higher risk of coronary perforation [28]. Nitrates generally should be avoided because they increase the angiographic degree of systolic narrowing and can lead to worsening of the symptoms. Surgical treatment with dissection of the overlying myocardium should be limited to patients with symptoms that persist despite medical treatment. Good clinical results have been reported in a small series of patients, although serious complications such as right ventricular perforation and left ventricular aneurysm are possible [29]. In the 2018 the Guideline for the Management of Adults with Congenital Heart Disease, in the section of Coronary Anomalies and Anomalous Coronary Artery Evaluation, relate to the Clinical Importance of anomalous aortic origin of the coronary artery and Risk of SCD. Referred intramural course of coronary artery into context of this coronary anomaly, don´t have any recommendation about this. The diagnosis of these an appropriate decision-making for the treatment of the symptoms associated with this CAA are not referred [30].
Conclusion
Myocardial bridging (MB) is a congenital coronary anomaly, generally considered to be a benign condition, it has been proposed as a cause of chest pain, coronary spasm, myocardial ischemia, acute coronary syndromes, left ventricular dysfunction, myocardial stunning, left bundle branch block and arrhythmias, and even sudden cardiac death. MB must be considered especially in patients at low risk for coronary atherosclerosis but with angina, like chest pain or established myocardial ischemia. The CCTA in patient with symptoms or conditions associated with MB are useful. Registries for incidental findings of MB in the CCTA and long term follow up don´t have performed. Medical therapy with beta-blockers and calcium channel blockers remain the mainstay of treatment. For select patient’s refractory to intensi?ed medical therapy, surgical intervention, or less preferably PCI with DES, can be considered.
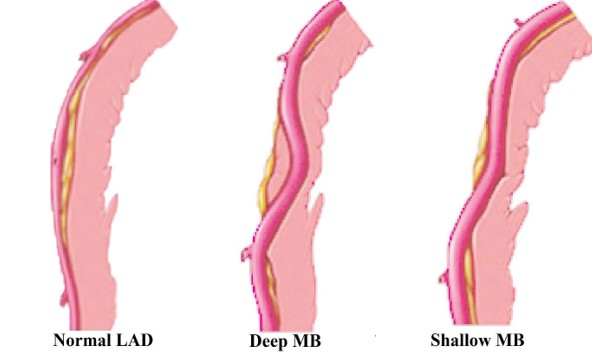
Figure 1: Illustration depicting normal coronary artery anatomy in LAD, deep MB and shallow MB in LAD. LAD: left anterior descendent artery; MB: myocardial bridge.
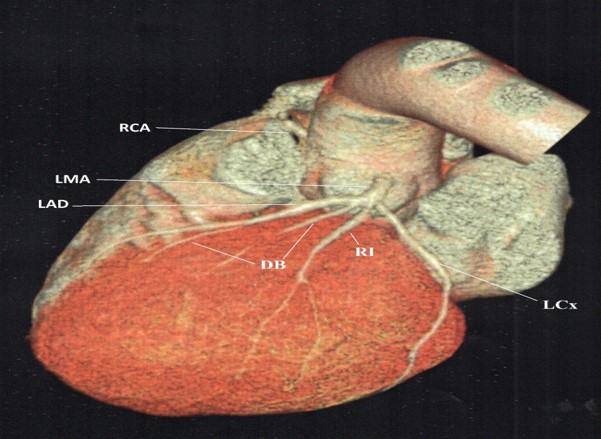

Figure 3: Additional analysis of the LAD MB in Figure 2 with CTTA. a) Cross-sectional view of intramyocardial course in LAD and View of an intramyocardial course in LAD (16,6 mm); Longitudinal view of intramyocardial course in LAD. LAD left anterior descending; MB, myocardial bridge; CCTA, Cardiac computed tomography angiography.

Figure 4: Coronary angiography showed a myocardial bridge (A) in middle segment of the left anterior descending coronary (green narrow) in a patient with angina and electrocardiographic changes.
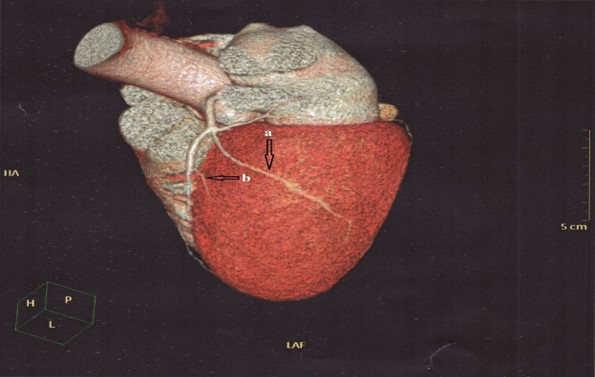
Figure 5: Cardiac multislice angiotomography: Coronary artery calcium score was 0. Left anterior descending artery without atherosclerotic lesions. A) Showed in Ramus intermedius artery of moderate size with a deep intramyocardial course (MB). B) The first diagonal artery without atherosclerotic lesions with intramyocardial course in distal third (MB). Circumflex artery, without lesions Right coronary artery dominant without lesions. MB, myocardial bridge.
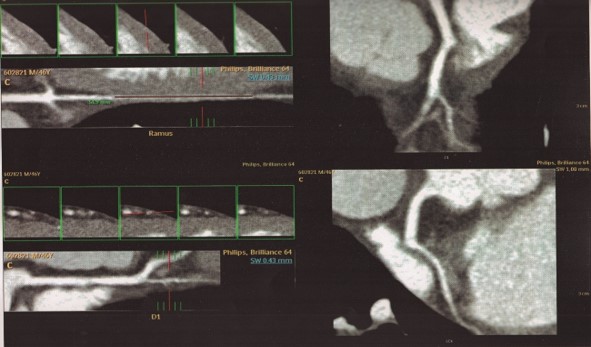
Figure 6: Additional analysis of the myocardial bridge in the ramus intermedius artery and first diagonal artery showed in Figure 4 with CTTA. Cross-sectional view in an extended intramyocardial course (MB) in RI artery (51,9 mm); and in the first diagonal artery. CCTA, Cardiac computed tomography angiography; MB, myocardial bridge; RI, ramus intermedius.
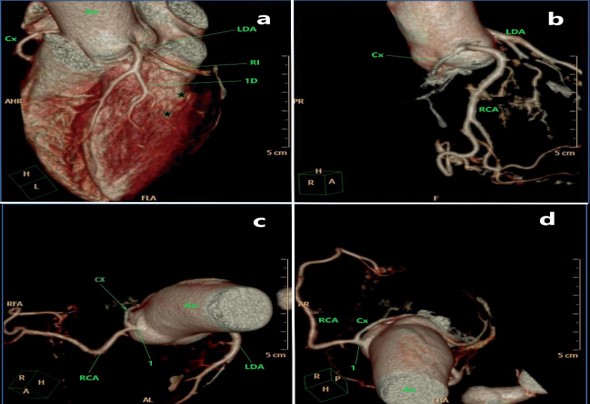
Figure 7: Coronary computed tomography angiography. Calcium score was 0. Showed the presence of Myocardial bridges (MB) in ramus intermedius artery, and MB in the first diagonal branch artery (asterisk). The presence of ectopic left circumflex coronary artery (Cx in green) arising from the proximal part of the right coronary artery (RCA) and single right coronary ostium (RCO). MB, myocardial bridge.

Figure 8: Analysis of the ectopic Cx showed in the Figure 6 with CTTA. A) Longitudinal view shows the course of anomalous aortic origin of a Cx arising from the inappropriate sinus (right coronary sinus) (green arrow) B) Longitudinal view shows the course of Cx goes backward and to the left, circling the aorta from behind, then passing between the posterior aortic wall and the anterior right atrial wall. LCx, left circumflex artery; RCA, right coronary artery; Cx, circumflex artery; CCTA, Coronary computed tomography angiography.
Citation: Ibarrola M (2020) Myocardial Bridges a Review of the Imaging Studies for Diagnosis. Ann Med & Surg Case Rep: AMSCR-1000033
