
Emergency Medicine and Trauma Care Journal
Case Report
Hyperkalaemia Induced Narrow QRS Complex Complete Heart Block
Rahmani SH1, Faridaalaee G2, Dehkharghani MZ3 and Pourya Pouryahya4,5*
1Imam Khomeini Hospital, Emergency Department, Urmia University of Medical Sciences, Urmia, Iran
2Amir-al-momenin Hospital, Emergency Department, Maragheh University of Medical Sciences, Maragheh, Iran
3Shams Hospital, Emergency Department, Tabriz University of Medical Sciences, Tabriz, Iran
4Casey hospital, Emergency Department, Monash Health, Victoria, Australia
5Faculty of Medicine, Nursing and Health Sciences, Monash University, Victoria, Australia
*Corresponding author: Pourya Pouryahya, Faculty of Medicine, Nursing and Health Sciences, Monash University, Victoria, Australia, Tel: +61 (03) 8768 1869; E-mail: Pourya.Pouryahya@monashhealth.org
Citation: Rahmani SM, Faridaalaee G, Dehkharghani MZ, Pourya Pouryahya (2020) Hyperkalaemia Induced Narrow QRS Complex Complete Heart Block. Emerg Med Truama. EMTCJ-100021
Received date: 18 December, 2019; Accepted date: 24 December 2019; Published date: 01 January 2020
Abstract
Potassium is an important extracellular ion with an important role in the myocardial cells function. Hyperkalaemia is a potentially life-threatening electrolyte disturbance which can impair cardiac conduction. Here, we report a case of a 72-year-old woman with past medical history of chronic kidney disease secondary to insulin dependent diabetes, who was brought to the Emergency Department with unresponsiveness 15 minutes after acute dyspnea. On arrival, the patient was in asystole without any cardiac output. Cardiopulmonary resuscitation (CPR) was commenced immediately. In addition to the resuscitation guideline during the CPR, with the presumed Hyperkalemia, treatment was started empirically while awaiting point of care electrolyte result. After treatment and during 3rd cycle of CPR, ECG demonstrated sinoventricular rhythm with ROSC. QRS subsequent narrowed down in her ECG followed by narrow QRS complete heart block within 15 minutes. Minutes later, she gained consciousness. Pathology demonstrated potassium level of 7.8 mEq/L and hemodialysis was scheduled. 2.5 hours post urgent hemodialysis, her ECG normalized to the sinus rhythm. She was admitted into the High dependency unit for ongoing management and was discharged home without any neurological sequalae after 12 days. This case demonstrated the wide variety of signs and symptoms as well as ECG changed secondary to Hyperkalaemia.
Keywords: Complete heart block; Hyperkalaemia; Hemodialysis; Narrow QRS complex
Introduction
Potassium is an important extracellular ion with an important role in the myocardial cells function and any change in the concentration may have a significant effect on the myocyte electrophysiologic gain [1]. Hyperkalaemia is a potentially life-threatening electrolyte disturbance and defines as a serum potassium levels greater than 5.5 mEq/L in adults. Significant hemodynamic and neurologic consequences can occur in the levels more than 7 mEq/L, whereas levels greater than 8.5 mEq/L can contribute to a respiratory paralysis and cardiac arrest [2]. Hyperkalaemia is often asymptomatic, when the symptoms present, they are nonspecific and most related to muscular and cardiac function. Diagnosis usually is based on the laboratory test and the confirmatory blood test should be done before commencing the Hyperkalaemia treatment in a patient without any predisposition, unless significant ECG changes consistent with hyperkalemia are present. Hyperkalaemia can be associated with a wide variety of ECG abnormalities from a tall, “peaked” T waves, shortened QT interval and prolonged PR interval to the widening of the QRS complex and a “sine wave” configuration and death [3]. High serum potassium concentration can contribute to conduction impairment in the Purkinje systems and ventricles more than in the AV node; however, complete atrioventricular block is possible and all these abnormalities have a good response to Hyperkalaemia treatments [4].
Case presentation
A 72-year-old woman (BW: 80 Kg) with past medical history (PMH) of chronic kidney disease and hypertension secondary to 20-year history of diabetes which for the past 5-year required insulin therapy, was brought to the Emergency Department with acute dyspnea and loss of consciousness 15 minutes prior. On arrival, she was unresponsive and apneic without any cardiac output, and her cardiac monitoring demonstrated asystole with the bed side blood sugar level (BSL) of 438 mg/dl (24.3 mmol/L).
Cardiopulmonary resuscitation (CPR) according to the resuscitation guideline was commenced with bag valve mask and 100% Fi O2, followed by crash intubation to control her airway. During the first minuets of resuscitation, she remained in asystole; however, at the end of the third cycle, return of spontaneous circulation (ROSC) was obtained and her cardiac monitoring revealed a rhythm with widened QRS complexes in a sine-wave configuration (sinoventricular rhythm). With regard to the rhythm and the patient’s PMH, empirical treatment for hyperkalaemia with calcium gluconate (10 ml of 10% solution) as well as 8 unites (0.1 U/kg) of short acting insulin (Actrapid) were commenced intravenously, due to lack of availability of any urgent bed side electrolyte measuring equipment, in particular potassium level, as well as point of care venous blood gas (VBG) machine. Because of her High BSL, it was decided not to proceed with 50% Dextrose water in addition to actrapid. Her QRS complex narrowed down subsequently (Figure 1) with BP 182/112 mm/Hg and Oxygen saturation of 95% (on 100% FiO2).
Continuing management with two more doses of calcium gluconate and insulin, the cardiac rhythm changed, and her 12 lead ECG revealed a complete heart block with narrow QRS complexes at a rate of 34 beats per minute after 15 minutes (Figure 2). A femoral catheter was placed, and she was prepared for urgent hemodialysis after pathology demonstrated potassium level of 7.8 mEq/L.
At this stage, she was awake and obeying command with HR 45 bpm and BP 134/92 mm/Hg, she was extubated successfully. Surprisingly, after 2.5 hours of hemodialysis without heparin, the rhythm changed to the sinus rhythm (Figure 3).
Exploring further, there was a 5-day-history of hospitalization in her PMH due to palpitation and weakness with diagnosis of hyperkalemia induced atrial fibrillation with slow ventricular response, which was managed medically without hemodialysis.
Laboratory data subsequently demonstrated: white blood cell counts of 22.100 × 103/µL (38%neutrophils, 58% lymphocytes and 4% mixed cells) and hemoglobin of 11.6 mg/dL. Her serum blood urea nitrogen (BUN), creatinine, sodium, and potassium concentrations were 135mg/dL, 4.4mg/dL, 137 mEq/L, and 7.8 mEq/L respectively. Total calcium level was 8.2 mg/dL and magnesium level was 1.8 mg/dL. Coagulation studies, including prothrombin time and activated partial thromboplastin time were normal.
She was admitted into the High dependency unit (HDU) after hemodialysis and underwent daily hemodialysis along with medical therapies. During admission, potassium level, cardiac rhythm, and level of conciseness remained stable, and she was discharged home without any neurologic sequalae after 12 days.
Discussion
ECG changes in hyperkalemia correlate with the level of the potassium. Early changes typically seen at the level of 5.5-6.5 mEq/L and include:
The progressively widened QRS eventually merges with the T wave, forming a sine wave pattern which follows with ventricular fibrillation or asystol5.The classic ECG manifestations sometimes are absent even in a sever hyperkalemia; therefore, ECG is not reliable for ruling out the hyperkalemia or monitoring therapy [6].
Hyperkalaemia induced complete AV block without QRS prolongation is a rare condition. It can be responsible for a wide range of ECG abnormalities. It produces a gradual depression in the excitability and the conduction velocity of the specialized pacemaker cells and the conducting systems4.Now the most current guide lines of hyperkalemia believe that the treatment should be commenced in the serum potassium levels more than 6.5 mEq/L, or with the appearance of the ECG changes [7].
Kim N-H, et al in 2005 reported, a 77-year-old woman with a 3-hour-history of dyspnea and dizziness before arrival. On arriving, her blood pressure was 80/40 mm Hg, with a regular pulse rate, and the ECG revealed a third degree atrioventricular block (AV) with a ventricular rate of 33 beats per minute. With regard to her vital signs, temporary percutaneous pacing was attached immediately and caused to the hemodynamic stabilization. The laboratory data showered a serum potassium of 8 mEq/L, urea nitrogen of 46.62 mg/dL, and creatinine was 3.22 mg/dL. With hyperkalemia medical treatment, blood potassium level decreased to 5.03 mEq/L after 2 hours and the ECG exhibited normal sinus rhythm [4].
Baratloo A, et al in 2014 reported, a 62-year-old man with a history of diabetes and ischemic heart disease, who was admitted in the emergency department with a 2-day-history of generalized weakness, nausea and frequent vomiting. On arrival, he was alert with complaining of moderate pain in the left hemithorax along with a cold sweating which had been present for the previous 3 hours. He had a history of hospital admission due to raised blood urea nitrogen and creatinine which was treated with one-time hemodialysis in the last year. The patient was unstable with a blood pressure of 75/55 mmHg and a pulse rate of 28 beats per minute. ECG revealed a complete heart block, thus transcutaneous pacing was attached immediately. Laboratory examination showed the potassium and creatinine levels of 8 and 5.13 mg/dL respectively. In addition, arterial blood gas revealed a PH of 7.23 with a PCO2 of 29.5 and HCO3 of 12.2. Calcium gluconate 10% infusion contributed to dramatic heart block elimination. They prepared him for hemodialysis and admitted him to the CCU ward [8].
Ohmae M, et al in 1981 reported, two cases of heart conduction abnormalities due to hyperkalemia. The first one had a complete heart block and second one had a right bundle branch block which both disappeared with correction of the hyperkalemia. They conclude that hyperkalemia can depress conduction in the His-purkinje system and subsequent complete heart block distal to the atrioventricular junction [9].
Tiberti G, et al in 1998 reported, a case of hyperkalemia induced complete atrioventricular block with unwidened QRS complexes which disappeared with effective hyperkalemia treatment and temporary endoventricular pacing. They conclude that temporary endoventricular pacing was essential in restoration of adequate renal blood flow and excretion of exceeding serum potassium and normalization of cardiac conduction along with hyperkalemia treatment [10].
Hyperkalemia is a common electrolyte disturbance that can cause some life-threatening dysrhythmia as ventricular fibrillation and asystole and some cardiac conduction abnormalities as complete heart block. Fortunately, this lethal imbalance and ECG abnormalities usually have a good response to early and effective hyperkalemia treatment as our patient and another.
Conclusion
This case demonstrates the wide variety of signs and symptoms as well as ECG changes secondary to Hyperkalaemia.
Acknowledgements
Special thanks to all staff of the Emergency Department of Imam Khomeini Hospital in Urmia.
Ethics
Written informed consent was provided by patient for publishing this case and any accompanying images.
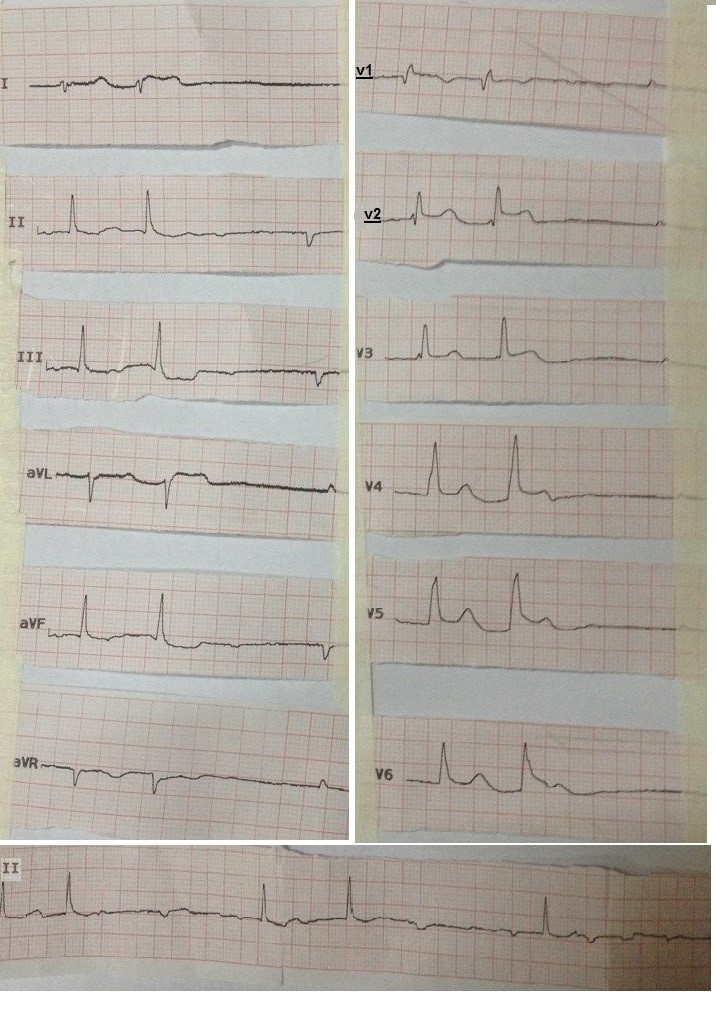
Figure 1: Narrow QRS complexes rhythm after first gluconate calcium injection.
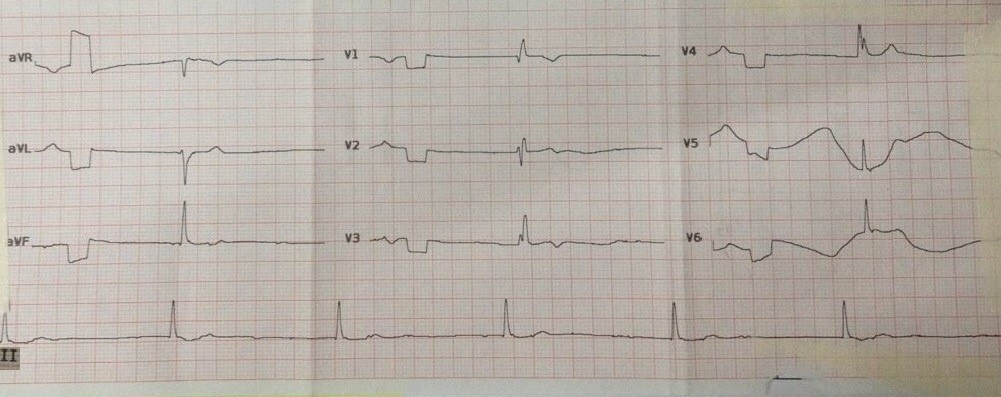
Figure 2: Complete heart block with narrow QRS complexes after hyperkalemia medical therapy.
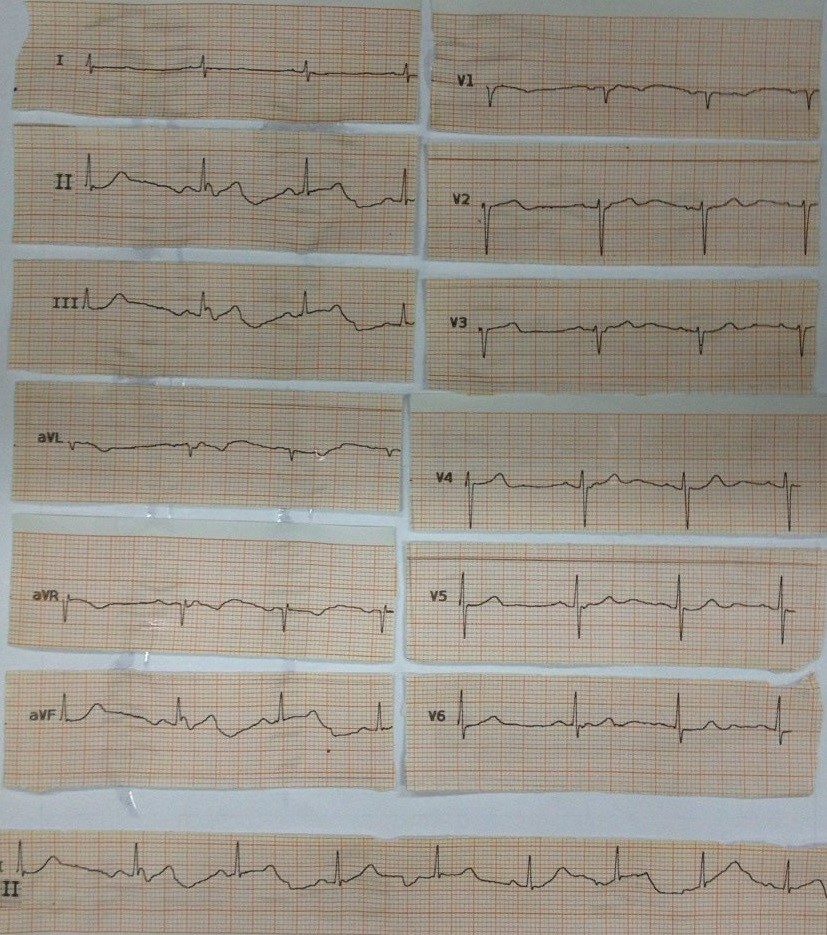
Figure 3: Sinus rhythm after hemodialysis.
Citation: Rahmani SH, Faridaalaee G, Dehkharghani MZ, Pourya Pouryahya (2020) Hyperkalaemia Induced Narrow QRS Complex Complete Heart Block. Emerg Med Truama. EMTCJ-100021
