
Annals of Pediatrics and Child Care
Case Report
Sonographic Diagnosis of Perforated Meckel’s Diverticulum Due to Ingestion of Button Battery
Zefov V1, Abdelrady FAZ1*, Jaber G2 and Ghazalah MA2
1Department of Pediatric Radiology, Latifa Women and Children Hospital, UAE
2Department of Pediatric Surgery, Latifa Women& Children Hospital, UAE
*Corresponding author: Abdelrady FAZ, Department of Pediatric Radiology, Latifa Women and Children Hospital, UAE, Tel: +971 4 219 3000; Email: abdelrady81@gmail.com
Citation: Zefov V, Abdelrady FAZ, Jaber G and Ghazalah MA (2019) Sonographic Diagnosis of Perforated Meckel’s Diverticulum Due to Ingestion of Button Battery. Ann Pediatr Child Care: APCC-100009.
Received date: 11 October, 2019; Accepted date: 15 October, 2019; Published date: 21 October, 2019
Abstract
Foreign body Ingestion is common in pediatric age group. Usually it passes with no consequences, but in some cases it might be retained in the lumen of esophagus, stomach, intestinal loop, appendix or Meckel s” diverticulum. Particularly dangerous is the swallowing of button battery, leading to severe complications. Accurate diagnosis of lodged foreign body is crucial for early management, and prevention of further complications. The diagnostic arsenal includes conventional radiographs of chest and abdomen, CT and Endoscopy. In our case, we emphasize the role of US as a safe, simple, quick as well as an accurate method for diagnosis and identification of Button battery in Meckel’s diverticulum
Keywords: Button battery; Foreign body ingestion; Meckel’s diverticulum
Introduction
Meckel’s diverticulum (MD) is identified in 1.2-3% of the population. It results from the failed involution of the Omphalomesenteric duct, which usually obliterates between 5th and 7th week of fetal life. Most of people with Meckel’s diverticulum remain asymptomatic. Around 5-10 % develop symptoms that prompt medical attention [1]. In pediatric age the most often symptoms are bleeding per rectum, intussusception, pain in lower abdomen. Very often, it mimics appendicitis. Foreign bodies (FB) ingestions are common in pediatric age group with wide varieties of size, shape and material of the FB. Most of children are toddler and the most vulnerable children are those with developmental delay. Approximately 3% of all FB ingestions are small button battery (BB). Probably the number of ingestions in children is bigger, as the production of sophisticated automated toys with BB increases drastically in the last decades. The Gastrointestinal tract is the most common place for FB retention but the MD appears the most uncommon place for (BB) lodgment. There are few previous reports of BB lodged in a MD but without characteristic sonographic diagnostic signs. We present a case with BB lodged in MD, complicated with perforation and sent to our institution with diagnosis acute appendicitis.
Case report
We present a case of 3 years old boy with lower abdominal pain, swallowing BB, sent to our institution to R/O Acute appendicitis. The conventional Radiographs of chest and abdomen supine position from previous hospital show two BB located in lower abdomen (Figure 1A), the bigger sized battery appears at level of ileo caecal valve, surrounded with soft tissue mass suggestive of attempting ileocolic intussusception or per appendicular mass. The erect position (Figure1B) shows air fluid levels suggestive of incomplete bowel obstruction. The lateral view (Figure1C) shows anterior location of the bigger BB raising the possibility of lodgment in MD and the patient was sent for abdominal sonography for precise localization of BB whether it is in the terminal ileum, appendix or MD. The abdominal sonography revealed normal size and echotexture of the appendix (diameter was 5 mm) with no BB in the lumen (Figure2A). The further scanning discovers a tubular structure with typical pseudo gestation sac sign, surrounded with redundant echoic omentum suggestive of inflamed MD probably perforated (Figure2B) With mild tilting of the transducer, the arching hyperechoic outlines of BB was visualized. The final diagnosis was BB lodged in MD and the patient was sent directly for surgical removal without any further investigations. The surgical specimen shows corroded BB out of the tip of perforated MD (Figure3).
Discussion
BB represent a distinct injury risk when ingested. Sodium hydroxide and hydrochloric acid appear at the cathode (negative) and anode (positive) ends respectively, leading to pH changes around the terminals. Such production leads to liquefaction necrosis and tissue injury [1] the age is an important predictor of severity. All fatalities and 85% of major effects are in children who are younger than 4 years. A major effect or death occurred in 12.6% of children who were younger than 6years and ingested 20-to 25-mm batteries [2]. The lithium alkaline battery produce more severe tissue damage compared with the BB because the lithium battery has higher voltage of 3V. The experiments with dogs show necrosis of esophageal epithelium 15 min. after fixation of battery deep to the inner muscular layer [3]. It is obvious how important is the timing management of MD with lodged BB. Time-consuming exams are not necessary. Our decade experience with sonographic diagnosis of MD using the sonographic pseudo gestation sac sign shows -sensitivity 87.1%, specificity82.1percentage, positive and negative predictive values for MD are 84.4 % and 85.2% respectively [4]. Our presented case proves once again the validity of sonographic pseudo gestation sac sign for precise diagnosis of MD. Patients who ingest button batteries should have an initial roentgenogram to determine the location of the foreign body. If the battery is located in the esophagus, urgent extraction is advisable. If it is located in the stomach, extraction within 24 hrs is necessary. If the battery has passed distal to the stomach, the patient needs follow up with serial roentgenograms. When the battery location does not change and peritoneal irritation appear, an operation is the next step [5].
Conclusion
Timing management of MD with lodged BB (extremely rare) is essential for the outcome. Despite rarity, such combination is real and always should be considered in differential diagnosis. The sonographic pseudo gestation sac sign is reliable diagnostic tool for precise diagnosis of MD. It complies with international efforts for “Image Gently”.

Figure 1A: Abdominal radiograph, supine position. The larger BB is located at level Ileocecal valve, surrounded with soft tissue density toward the caecum mimicking attempting ileo caecal intussusception or large periappendicular mass.

Figure 1B: The erect position of abdomen shows air fluid levels suggestive of incomplete small bowel obstruction.
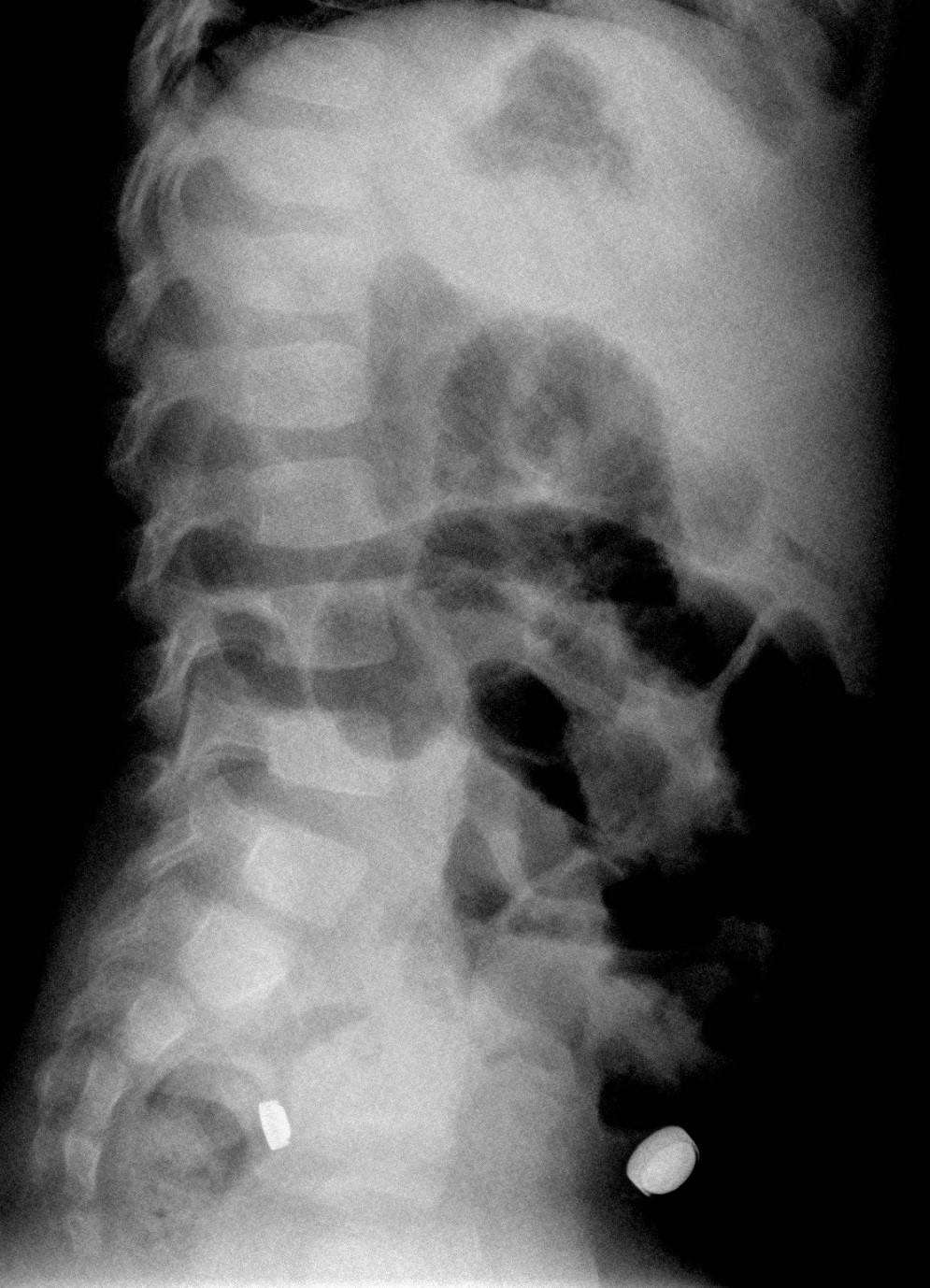
Figure 1C: Lateral view of abdomen. The larger BB appears anteriorly located which prompted sonographic exam for exact location.
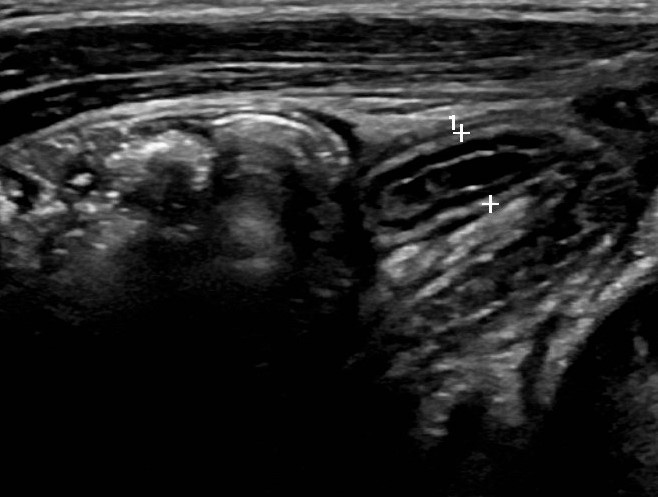
Figure 2A: abdominal ultrasound, the appendix appears with diameter 5 mm and normal outlines. The suspected variant of acute appendicitis with periappendicular mass is negative.

Figure 2B: Medial to the normal appendix, a tubular structure with Pseudogestation sac sign is seen (arrows) surrounded with hyperechoic omentum suggestive of inflamed Meckel’s diverticulum.
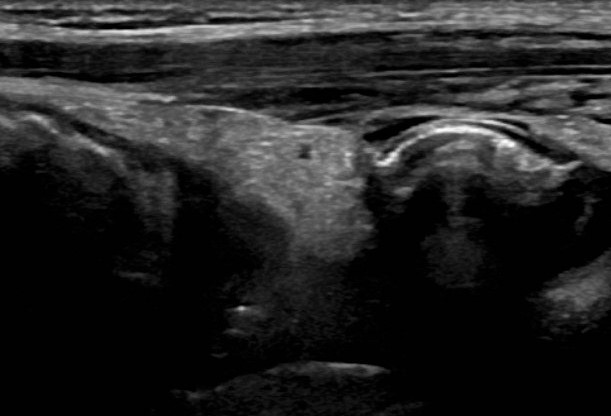
Figure 2C: With mild tilting of transducer, hyperechoic arch of the BB metallic outline appears with acoustic shadowing.

Figure 3: Resected Meckel’s diverticulum with gangrenous tip and corroded BB.
Citation: Zefov V, Abdelrady FAZ, Jaber G and Ghazalah MA (2019) Sonographic Diagnosis of Perforated Meckel’s Diverticulum Due to Ingestion of Button Battery. Ann Pediatr Child Care: APCC-100009.
